Covid is one aspect of this. Another is the massive. underfunding of the NHS over the last decade. This has become much more evident post-covid thanks to the backlogs.
- Getting a GP to see you in person is now quite difficult (they want to do everything via phone).
- Seeing your GP (depending on your area) can involve a 2-3 week wait and waiting in an hours long phone queue.
- When you are referred to hospital for tests you can be waiting 6-12 months for the most simple things if they’re not life threatening (even if they are life limiting in the meantime).
I personally have gotten to the point where I would not want to live in this country without access to private healthcare. I’ve had a number of treatments privately and they’ve saved me months of pain, anxiety, and in one case outright refusal for treatment by the NHS until the issue became dangerous (which was inevitable).
In the UK we treat the NHS like a sacred cow. Even people who have experienced appalling treatment feel the need to exonerate the NHS when complaining about their experience. While the people that work there are not the problem (the failures of the government are) we need to start calling a spade a spade. The current condition of the NHS is atrocious. It’s not “great/the best health system in the world” and we’re no longer “so lucky to live here with the NHS”. It’s shit and it needs massive changes. Unfortunately without a change in government we’re not going to get those and people are seemingly more concerned about refugees arriving by dinghy than health care.
Price inelastic healthcare is a private equity dream. The project to leave NHS funding unreformed in order to buy acquiescence to its sell off, all the whilst leaving people to rot, is to my eyes scandalous. But somehow unremarked in the twilight zone that the UK has become.
The UK media is an example of an oligarchy successfully controlling the entire information landscape and consistently pushing for manufactured “problems of the week” while ignoring real disturbing trends in home ownership, poverty, health and inequality between London and the abandoned “regions”.
The book “Fake law” was terrifying to me - it talks about a whole number of high profile judicial cases that were pretty much distorted by the Mail/Times/Telegraph into whatever propaganda they wanted to push that week, often directed just in ways that it would benefit the oligarchy. And there are multiple books like that. Fake Law, Flat Earth News, Merchants of Doubt.
The Guardian is ok but it doesn’t have the staff for real investigative journalism or long form. There’s a reason why the big breaks journalists got in the last decade or so were whistleblowers delivering them data dumps, not journalists following up a story - Flat Earth News talks about this - newspaper staff has been gutted to the point where that sort of thing doesn’t exist anymore.
And without that staff, The Guardian can’t do proper investigations on london real estate’s connection with major money laundering for instance.
Indepedent like someone else pointed out is owned by a Russian oligarch. BBC doesn’t have the mandate to do investigative deep journalism, they can only do reports or documentaries - but that BBC can’t break a major story or investigate anything of political importance because that would jeopardise their “apolitical” position.
This leaves the right wing media, which is the majority in the UK (opposite to the US, in the UK the right wing dominate the media) and they manufacture and manipulate the stories into seemingly-real controversies that are actually just a cover for them to get some law or change passed in Westminster. Read the book “Fake Law” - the way the Mail/Times/Telegraph have distorted even simple judicial cases into something they could use to get popular support for whatever their owners wanted is profoundly disturbing.
I don't. The Mail wants to turn every story into outrage. The Telegraph has lost touch with reality, and is frankly weird. I cancelled my Times subscription over the weird reporting of the Snoopers Charter. I checked back recently and it has just got worse
No, he's right. And it has been this way for a long time. The way Corbyn and Assaange were demonized and smeared ought to have made it obvious - but that's the thing about controlling the entire media landscape. Even if it ought to be obvious, there are people telling you to ignore the truth tellers, and you've nowhere to read their exposes except social media, where in fact they are likely shunted down the algorithm.
There are always people running in online to say that since "both sides" detest the BBC they must be doing something right, but that's ignorance at best, if not plain disingenuous. The BBC have an insanely pro corporate pro war stance, and have wielded it in elections with craft and force. Same w the others.
It's not just me saying all this either. Many have noticed. Many decry the loss of a balanced media landscape. But you won't hear about it on corporate news, or the Beeb or the Grauniad either.
Yes but apparently a bit of very real antisemitism is a small price to pay for having the left wing of capital in power instead of the right wing of capital.
Unfortunately the anti-semite line was easy to make stick because of his well known vocal opposition to the Israeli oppression of Palestinians. So not an incredible feat, but it was a case of corporate interests and the Tory party pushing the "emergency button" as an real Social Democrat was getting too popular and very close to becoming PM.
Also, as seems to be the fashion for left wing politicians, he has a soft spot for Russia. I think some people still think there is a Communist utopia over there, it's very strange. Not a good look recently.
I don't believe that there would have been no response from the UK to the Russian invasion if he had ended up PM, but it would have been slower and less impactful.
No it wasn't. Tremendous coordination and force went into pushing that line.
> because of his well known vocal opposition to the Israeli oppression of Palestinians
A view shared by right thinking people everywhere. Oppression is bad yo.
> it was a case of corporate interests and the Tory party pushing the "emergency button" as an real Social Democrat was getting too popular and very close to becoming PM.
Yes. But it wasn't easy, and it wasn't right, and the fact that the BBC and the Guardian and every other major paper and network failed to call the smear campaign out - and even fed it - is indicative of horrifying and deep problems.
> as seems to be the fashion for left wing politicians, he has a soft spot for Russia
Not really, he just isn't into escalating into war with a nuclear power; and recognizes that the Russian people are not the Russian leadership. This "nuance" has been shot and buried in a shallow grave.
> I think some people still think there is a Communist utopia over there, it's very strange.
Literally no one is saying that, except for corporate right wing media putting words in people's mouths. It's really weird that you'd believe them, given - again - that no one is saying that, or anything even remotely like it.
> I don't believe that there would have been no response from the UK to the Russian invasion if he had ended up PM, but it would have been slower and less impactful.
Again, this is a line pushed by right wing corporate media against left leaders all the time. And I thoroughly disagree with it.
Like - how is BoJo faring right now? Do you feel he's respected as a leader? Come off it.
And Britain is on the brink of blackouts without Russian oil, thanks to the dependence on oil fostered by Tories and their mates. A left, pro environment government would not have been so dependent in the first place.
>No it wasn't. Tremendous coordination and force went into pushing that line.
There is no need for coordination when Corbyn did nothing but feed the news cycle with stupid acts and dumb hot takes.
He also directly supported and appeared on stage with people who are anti semites and just did everything possible to be guilty by association.
>And Britain is on the brink of blackouts without Russian oil, thanks to the dependence on oil fostered by Tories and their mates. A left, pro environment government would not have been so dependent in the first place.
Being on stage with known anti semites, supporting known anti semites (for other reasons), appearing on Iranian state TV and blurbing one hot take after another.
The UK reliance on Russian fuels was less than 3% of total imports the vast majority of which were through mixed fuel imports from the EU.
There were no direct import contracts between the UK and Russia.
> is to my eyes scandalous. But somehow unremarked
There's a lot of remarking going on - Private Eye, for example, have been banging the "NHS privatisation" drum for a couple of decades at least. The Guardian, too, mention it not infrequently.
This is very true. The NHS has become a commissioning organisation -- it puts out a request for a service and providers bid for it. Many of these services are IT related; many of them are things like physiotherapy referral programmes. Patients may or may not know who provides their care. This is not at all how things used to be and I have noticed it get far worse of late.
As an aside, I’ve had first hand experience in a couple of those outsourced IT services and the amount of wasted money in that area alone is staggering.
"At the moment, UK public health spending is the equivalent of about 7% of GDP, similar to what it was back in 2010 and higher than in previous years. Back in 1955, it was worth about 3% of GDP."
If the NHS quality of service is as poor as I hear, after decades of increases in funding, why on earth do I also hear it referred to as a "beloved public institution"? Is that just something people feel they are required to say?
So they spend slightly more than double what they did in 1955, when the cost of providing healthcare has gone up nearly 4x due to the Beaumol effect. That doesn't seem good? You'd expect the service to gradually get worse in that case, wouldn't you?
Double in GDP terms means a massive increase in real terms because GDP is so much higher now. Our GDP in real terms has increased 5x in that period, so double funding relative to GDP is a 10x real terms increase.
The point from an affordability perspective is, has NHS funding relative to GDP actually fallen since the end of the last labour government? The answer is no, it’s about the same.
Now it’s reasonable to argue we should be spending more of our GDP on health care, but we’re in the middle of a major global inflation crisis. The recent rise in NI which partly funds health care was slated by the left. How is the country going to afford a significant increase in health spending right now?
So why should the Baumol effect apply so heavily to healthcare? It's true 1 on 1 patient care has limited options to increase productivity, but is that sufficient to explain it?
The NHS is also under huge pressure because of all the European health care professionals that left after Brexit (you won't read about that in the Telegraph) and the huge number of sick days caused by COVID.
I also feel they are way too quick to dismiss the idea that health issues are related to COVID. When kids were vaccinated against measles the death rate fell not just for measles, but for all infectious diseases. It's probably because measles damages the immune system. It's not unlikely that COVID had long term health effects that we don't yet fully understand, but which are starting to show up in the statistics.
You are mixing figures here, OECD stats are for healthcare expenditures the UK currently spends about 12% of its GDP on healthcare and is aligned with most developed economies.
This is different to NHS funding alone.
Also comparing the UK where healthcare is predominantly a single payer system to countries like Germany isn’t apples to apples. Germany has a multi tiered private-public healthcare system and it’s not single payer.
Good point. But I can't make the numbers add up. If NHS is 7% and total health care is 12% then the NHS is only 58% of health spending, but how does it then make sense to say it's "predominantly single payer"? Looks to me like the private sector has exploded recently as people pay for private health care/insurance to cover the increasing gaps in the NHS coverage. This does nothing for those who are still just on the NHS.
This looks to be backed up by: "Based on trends observed in early estimates of household final consumption expenditure, household spending on outpatient and hospital services, which include self-funded and insurance-funded treatments, grew by 24.5% and 31.3% respectively in 2021." https://www.ons.gov.uk/peoplepopulationandcommunity/healthan...
But that link also says that NHS spending is 83% of health spending, so like I said I can't get the numbers to add up.
Perhaps for some reason your friends are disproportionately feckless cowards? I've met zero people in my life who have any fear of criticizing health systems, public or private. Perhaps the people I've met are just unusually heroic.
And so your aunt is currently able to purchase a higher quality of care because she has the money to do so? And this is an option for all moneyed citizens of the UK?
While I'm not a fan of your tone (not that of your parent poster), I agree entirely with the bones of your post. I do not think their experience as stated is anywhere near... universal.
Indeed, I'll admit my tone can get quite peevish after reading for the Nth time about how people are being silenced (note the irony there). It's nothing other than trying to create a victim/persecution complex to sell your point of view and it's an intellectually low tactic.
You wouldn't know, would you, with an attitude like that? Look at this thread. "The NHS is a national religion" is a cliché because it's true. There are loads of comments saying people are irrational about it. The country has too many people who melt down and viciously attack anyone who tells the truth - the NHS is a crap idea, always was and needs to be abolished. Go canvassing in the North with that idea and see what happens.
Indeed; the reason people exonerate it is that the Tories have been threatening the population with a dismantling and privatisation of the NHS for over a decade now, and that's not what anyone wants. People want the NHS to work, to be funded and managed appropriately. A primary reason it doesn't is the Tories crippling it.
The NHS has been turned into what is effectively a state religion in some quarters. It's untouchable. It can't be criticised. It's immune to meaningful improvement and reform at this point. Yet everyone I know who works for the NHS has a litany of stories about the inefficiency and waste. And it consumes an increasing proportion of the GDP. Eventually, something will have to give.
Its been on an unsustainable path since its inception. It's always been in crisis and needed increasing amounts of cash. Cash that we taxpayers have no choice but to pay up. The NHS isn't optional, it's mandatory.
If we have the option to opt out of paying for the NHS and go private, many will do so. I already have to pay twice over. I pay privately through my employer's plan, and then again for the NHS. I suspect if there is the possibility of opting out and going entirely private, many would do so. At this point it's the only way to ever get a GP appointment for many of us.
The problem with the debate here is that it's always framed in terms of UK vs US funding models, both of which are horribly broken in different ways, and never looks at other European countries or other systems around the world, some of which have systems which work better and provide better health outcomes for less money. If we were to privatise it along French lines, for example, it might be a massive improvement all around. But that debate has never happened.
"I pay privately through my employer's plan, and then again for the NHS."
And yet it is the private system in the UK that is taking away scarce supply from the NHS making it more vulnerable.
There is a supply side limit on doctors and nurses, which means private healthcare works like the Fast Track queue at Alton Towers. All it does is allow people with money to jump the queue at the expense of everybody else.
And remember that since the inception of the NHS Primary Care, ie the GPs, have always been private businesses. Yet that is the bit that is completely on its knees at the moment.
This isn't a private vs public argument. It's far more fundamental than that. It how do we share out increasingly scarce resources in a country that is getting poorer.
> And yet it is the private system in the UK that is taking away scarce supply from the NHS making it more vulnerable.
It's not a system doing it. Healthcare professionals are choosing to work for private companies instead of the NHS. If you would like to ban that, then say so, but don't pretend there's an amorphous system to blame.
There is an amorphous system to blame - too much demand and not enough supply.
Some of that demand has money, therefore the private system will take capacity away from the NHS to supply the money. Of course it will.
That is jumping the queue.
Therefore as a society we have to ask whether we want to uphold the NHS's founding aim: "Healthcare free at the point of delivery based upon need not ability to pay".
We can't fix the supply shortage by taxing the rich. But we can stop the queue jumping by constraining who private healthcare is permitted to treat and in what order.
For the record I don't like the Fast Track queues at Alton Towers either. That's not the British way. In Britain we stand in line - whether Lord or Leper.
> how do we share out increasingly scarce resources
We make people pay for them. Like we do with every other resource on the planet.
Healthcare is something which should be accessible for all, and we can of course subsidise the less well off. But it still ultimately needs paying for.
The supply side limit is purely because the government chooses not to train sufficient staff. We have a government imposed cap to train 7500 doctors per year at University. Then when they finish, they do two years at FY1 and FY2 level, but there are not then sufficient places for all doctors to go onto a training programme. A friend of mine is applying for the January intake of anaesthetics this year for e.g. and there are something like 25 places in the entirety of the UK for that specialty. So people end up working as locums, working to fill gaps in rotas, which has a high hourly rate. Then, when they do finally manage to get a training place, they take a big pay cut and work more hours. That’s if we’re lucky - because plenty of them just go to Australia where the standard working week for a Dr is 40 hours, and many of them don’t bother coming back. But this is a problem created entirely by the government’s choices.
We also have a hugely archaic system in the Royal Colleges. In no other profession do we expect people to sit regularly very expensive professional exams, and expect the staff to fund them out of their own salary rather than them being funded by their employer. £600 a go is not unheard of.
"We have a government imposed cap to train 7500 doctors per year at University."
We do. And you know why. Because the NHS has no more capacity to train any more than that. In fact this last year it has struggled to do that because it was more interested in ensuring its staff had masks on properly than getting the job done. First year medical student placements in hospitals were the first to get the chop.
To train more people in any system, that system has to do less of what it is currently doing and more training. We can't afford that in the NHS, which is already struggling to meet demand.
Ultimately the problem is that we spent the seed cord in the 1990s, and we're struggling to replace it.
> It how do we share out increasingly scarce resources in a country that is getting poorer
In this instance, the resources are humans, and it seems you want to force humans to do something they don't want to do. If you want slave-doctors just say so. It worked for the Romans I guess.
Except it isn't an argument against nationalised healthcare. The UK has nationalised health care and that is what OP is complaining about. I think it would be more an argument by OP against "nationalised healthcare with legal private healthcare".
The exact argument is "doctors/nurses are limited, and they aren't behaving how I think they should behave. Let's fix the system so they have no choice". I guess that isn't slavery, that is just funneling people into a single path which they clearly don't like, because they reject that path when they have literally more than one option open to them.
It seemed like OP was arguing that private medical practices, which are still allowed in England, should be banned because they're using up all the "resources" the NHS needs (doctors/nurses).
I agree that a ban is ineffective. In lieu of a ban the NHS should raise their staffer's pay and fund the increase with financial asset and land taxes.
You are not paying twice over. Your private insurance is dramatically cheaper than it would be if it covered everything covered by the NHS.
You do have overlapping cover, but the most expensive cover (GP, long term chronic conditions, emergency care) are provided by the NHS. It’s far from clear that you would pay less if you had to cover the whole through a private policy.
I find this is a common and totally unjustified take. The NHS is fairly frequently subject to alteration and reform in various ways, and there is no real truth to the “piles of bureaucracy and waste” stories - it remains broadly pretty efficient as a healthcare system when compared with other developed countries.
You’ve also misrepresented the nature of private healthcare in the UK - this is almost universally not a replacement for NHS services. It will offer you things like faster GP appointments, consultants, and routine operations. It will not replace many of the specialist or emergency services offered by the NHS, leaving you dependent on it anyway.
A bigger “problem with the debate” is that we so frequently find people like yourself who are insistent on having some kind of “debate” without really knowing about what, or why.
All employer provided healthcare setups I have encountered in the UK do not even offer a GP replacement service [1]. You still need to go to your NHS GP and get an open appointment and then the insurer will redirect you to an approved service (where you will indeed get a faster appointment). Also most insurers do not cover most chronic problems (you'll have to fallback to the NHS) and are really meant to cover just acute issues.
edit: and of course you'll rely on NHS for any emergency.
[1] at least not without paying out of pocket for the significantly more expensive premium coverage. Some now offer phone consultations but you still need to go to the GP for referrals and prescriptions.
> You’ve also misrepresented the nature of private healthcare in the UK
I mentioned that we don't have the right to opt out of paying for the NHS. It's not possible go entirely private. If you could opt out, you could pay that money to a private provider instead and entirely forego the use of the NHS. That isn't an option today. But it should be.
I have private health care through my employer, I've only used it once but it was very handy. I don't agree with your take at all, there's no way a private health care outfit could efficiently provide an effective emergency service across the entire UK for all possible injuries and illnesses, completely replacing or duplicating the NHS. The USA has tried this and it's an incredibly expensive disaster.
Employed middle aged workers in the USA pay about the same as we do for the NHS to support Medicare, Medicaid and CHIP through taxes, and then have to pay about the same again to actually get health care for themselves. Plus the system that costs twice as much as ours per citizen still leaves tens of millions of Americans without health insurance. It's utterly godawful. Our current system where everyone supports the NHS, and if you want top up services you pay for it, ensures solid funding for everyone's health care. The fact that my private care actually subsidises the NHS by reducing demand on it is a feature, not a bug. There's also the fact that private health care increases overall investment in health care, so in emergencies the NHS can call on private medical facilities which otherwise wouldn't be available. I know there's a fairness argument, but in practical terms our system benefits everyone.
Yup, as an American this is a pretty accurate assessment for the most part. It's also worth noting that several states actually have different systems to close the gap for people who don't fit into the medicare-medicaid-chips safety nets. In California we have medical, which adds an extra tax, but does help a lot of people who would be uninsured get health insurance. Different states will have massively different levels of care and expertise available.
For what it's worth if you have the money you can get some pretty world class care here. My dad had cancer and due to my mom's really good (publicly provided mind you, she worked for the school system) insurance got my dad great care and he's still out an about to this day
And when you have a heart attack in the street, who's responding?
In this scenario, why should an NHS ambulance pick you up when you don't contribute?
Surely it should prioritize those on public healthcare?
Some poor lad whose leg is broken from a fall?
"opt out" is how conservative parties kill public healthcare systems.
Because the public healthcare system winds up subsidizing the private one: private insurers dump bad risks onto it when they get too expensive too insure, after years or collecting the payments that don't go to the public system.
It's the definition of privatizing profits and socializing risk.
You want to opt out? You get to opt all the way out. You don't get to come back, it's a one way street. Still keen?
I’m Germany, that’s the way it works, once you choose to go private you cannot opt back into the public system. People sometimes do it if they don’t plan to stay in Germany though, usually if they are immigrants.
Depends on the age. Above 55 it's indeed quite difficult, under that you can switch back if you fall back into the required status (i.e. take a job with a salary under the limit)
I think if you’re forced to go private due to long nhs wait times the money you have spent on paying for the nhs via your taxes should be refunded to cover private care cost
Why should it be an option? Because we live in a free country, and should be free to spend our money as we see fit. Even if others don't agree with it. Why should we all be compelled by the force of law to divert a huge fraction of our income to an organisation which is so ineffective and inaccessible?
We are forced to spend a significant fraction of our salaries on the NHS whether or not we want to. If we feel that this is not good value for money, or of poor quality, we don't have any real option of choosing to pay an alternative provider. Like all nationalised industries, it's inefficiently run because top-down administration of huge organisations blunts initiative and freedom of action. It's run by Whitehall and politicians, with little input from those actually doing the real work. And the result is that it's in perpetual crisis, with COVID having pushed it right over the edge. Is it really fit for purpose? I don't personally think so, and haven't for many years.
Competition is good for many reasons. It improves the quality and value of goods and services. The NHS has no real competition. There's no direct cost of failure, no direct cost to poor purchasing decisions, no direct cost for poor quality of service, and no real driving reason for improvement in the quality and efficiency of its services. They get the money anyway.
Other healthcare systems in Europe have fully private provision--you have the choice of where to take your money, even if you paid into a public system. If a particular hospital or clinic is providing poor or expensive service, you can take your money elsewhere which is better quality and better value for money. That's a very real incentive to drive improvement and efficiency. That is not the case for the NHS system. There is no choice, and the incentives to improve are minimal.
If there is to ever be any improvement in the NHS, there needs to be competition. The NHS should be somewhere you choose to have treatment because it's the best option, not because it's the only option.
Even though I agree with your comment, I don't know of any European countries where you could opt-out from paying social security. Even if some small eastern european country has this option, it is probably unsustainable for a larger country (or one with more healthcare spending).
It could be done multiple ways. You could pay into a government insurance scheme or you could pay into a private one. The main point is that the payment of the insurance premiums is decoupled from the service provision. Right now the two are tightly-coupled and you can't realistically choose either of them. Look at the French model as an example.
On a small scale, there is some degree of separation. Sometimes the NHS pays for treatment in private facilities, and sometimes private insurance pays for treatment in NHS facilities.
We've had privatisation experiments in English healthcare for years.
Dentistry is a fucking mess. Eye care is a fucking mess. Care and Nursing homes are a fucking mess. Large private provision of GP care? They can't do it and they hand the contracts back. Specialist commissioning in mental health? It's a fucking mess.
> It's run by Whitehall and politicians, with little input from those actually doing the real work.
If you say things like this it makes me think that you don't know that NHSEngland/Improvement is an arms-length-body, nor what that means in terms of command and control of the English NHS. It makes me think that you didn't know what CCGs were nor how they worked, and that you don't know what an ICS/ICB is nor how they work.
We've had privatisation experiments in English healthcare for years.
Dentistry is a fucking mess. Eye care is a fucking mess. Care and Nursing homes are a fucking mess. Large private provision of GP care? They can't do it and they hand the contracts back. Specialist commissioning in mental health? It's a fucking mess.
> It's run by Whitehall and politicians, with little input from those actually doing the real work.
If you say things like this it makes me think that you don't know that NHSEngland/Improvement is an arms-length-body, nor what that means in terms of command and control of the English NHS. It makes me think that you didn't know what CCGs were nor how they worked, and that you don't know what an ICS/ICB is nor how they work.
> If there is to ever be any improvement in the NHS, there needs to be competition.
What is "choose and book"? We tried competition, and it dramatically increased costs without doing anything at all to improve care. We're now spending considerable amounts of money rolling back some of that law.
Your dentist example is a bit weird - you're comparing private provision with NHS provision, and that doesn't work. If you want a private dentist, or a private psychiatrist, you pay and get rapid access.
If you can't afford private treatment you go on the NHS. At the moment NHS dentistry is simply not available for very many people. Those people cannot get treatment at all. But for psychiatry, the vast majority of people who need a psychiatrist will get same day or next day access. This is one of the problems - that's a statutory function, they must provide it, and so community care has been cut in order to meet the statutory function.
> Because that's the current wait time for an NHS psychiatrist.
This is untrue in the way that you've presented it. I'm not able to find this statistic any where - what's your source for it please?
There are long waits for some community mental health services, but these are mostly caused by decades of underfunding of MH treatment. Also, your argument says that this problem would be fixed with competition. We've competition and right to choose for first episode of mental health care since 2014[1] and that competition has done nothing to improve things and in many situations has made things worse.
For Early Intervention in Psychosis services (these are services for people with their first episode of psychosis) the current numbers[2] are that 83% of people were seen within 2 weeks after referral.
The number of people in contact with specialist mental health services has increased[3] since 2019 from 1.3m to 1.6m people. This is combined with a decrease in bed numbers and a complex change from CCGs to ICSs. New referrals data is complicated (one person can have multiple new referrals; someone already in contact with services can have a new new referral) but the trend is increasing[3]. The number of young people accessing MH services has increased a lot over the past 12 months, from 575,000 in Mar 2021 to 690,000 in May 2022.
Dentistry is a mess because of the funding model. It doesn't pay to be an NHS dentist, so most practices ceased to take NHS patients. If they fixed the funding model, the problem would resolve itself. The problem here was entirely self-inflicted by the NHS in its fixed price lists, which weren't sufficient to run a viable business on. The very opposite of a proper free-market economy. Finding an NHS dentist in some areas is impossible, but finding a private dentist is not. I've used both, and both were absolutely fine. The private dentist was more expensive, but they were charging a reasonable amount to fully cover their salaries, facilities and consumables. As with everything, you get what you pay for.
Regarding competition, the NHS hasn't really tried competition seriously now, has it? Not really. Not actually doing a complete decoupling the insurance funding and the service provision. The "choose and book" isn't that, is it? It's a small attempt, which is better than nothing, but it's not really surprising that it didn't drive a huge amount of change, when it's not really going to have a big impact upon the bottom line.
It wasn't intended to be so, but overall I do think that taxes could be reduced significantly. I do think that taxes are used inefficiently and that individuals are better at making decisions in their own and local interests in place of poorly-accountable bureaucracies. But I certainly am not advocating for not paying taxes at all!
I just don't know why that is, every piece of that puzzle I have met, was really efficient and generally doing a good job.
Spain is now trying to fix this and pensions by doubling self-employed tax. UK should probably follow suit, UK self-employed tax is ridiculously low. 20% on profits until 50k pounds won't cover a functioning healthcare system (or pensions for that matter).
What on earth? UK selfemployment tax is far more aggressive than this and the tax authorities have been on an aggressive campaign against selfemployed people for many years, leading loads of people - including me - to give up selfemployment and end up paying LESS tax as a result.I miss selfemployment! but it doesn't bring enough benefits to justify being reamed AND demonised.
And fuck the NHS. Smash the shit out of it. We'll all die exactly the same number of times without it, but be healthier and happier on the way.
I disagree with the threshold you mention. 50k£/year isn't exactly "rich", and even less so given the current conditions with regards to inflation, housing prices being through the roof, etc.
Governments shouldn't be providing anyone with pensions in the first place. Instead they should make defined contribution plans like IRA and 401(k) available to everyone.
Someone with the default tax code would take home £ 25,539.52 which means they pay 20.2% in tax. It’s quite low by many countries standards but certainly not 15%.
>that's not what anyone wants. People want the NHS to work, to be funded and managed appropriately.
No, they want cost-effective healthcare. Almost everywhere else in the world uses a mixed public-private model for healthcare, which IMHO keeps a lid on the excesses of government spending into the money pit of fully-public healthcare.
The UK spends less per capita (PPP) than most other equivalent country's health system [1,2]? I never quite understand the "cost effective" arguments against the NHS. These costs include all of our private health care expenditure, which are surprisingly significant.
The two are not mutually exclusive; you can pay less for healthcare than other countries, and still get a bad deal.
Eg: It's currently almost impossible to get routine or early-stage healthcare. If I want a routine doctor's appointment, I have to phone every day at 8am when the next batch of appointments are released, and hope I get one. Last time, it took hours on hold, and attempts over several days, to get one.
Your GP surgery is privately run, so in this case the issue is likely very much an issue of the supply of available doctors, and how your GP surgery chooses to operate its appointment system.
I believe appointments are now run more efficiently due to the backlog and changes in processes due to Covid, with the reason for an appointment usually submitted digitally first, followed by an efficient telephone consultation that is well prepared based on your submitted reason for needing an appointment, and a follow-up consultation as necessary. Perhaps your GP surgery in particular is struggling, or you are perhaps not engaging with the new approach.
I have been surprised at just how well functioning the health service is right now despite the incredible pressures on it, but perhaps my local area is coping better than others.
Importantly, however, this issue was broadly not present 10 years ago when the NHS was better funded to meet its needs, and was still cheaper than other countries. So the issue is not the NHS, but funding, which is also corroborated by our relatively low level of health spending.
The left has somehow ended up as the party of the political managerial class instead of the working class, this is one of the best explanations why we're in such a weird place where the socialists are all trust fund kids who would rather have the working class arrested than talk to them.
If the (UK) left is the party of the political managerial class, what is the (UK) right? When I'm feeling particularly sarcastic I might call them the party of dilettantes, but is that apt?
Oddly, things kind of flipped around (in very broad terms). The left is where some of the well-off urban middle classes are, along with the far-left socialists. The right is where the less well off but working are, along with some non-urban upper- and middle-class voters. Because for a lot of working class people (primarily those who work, and aren't living off state support), they have been entirely abandoned by Labour after being treated as guaranteed votes for decades. This is a big part of what the so-called "Red Wall" is. It's socially conservative (small "C") workers from traditionally Labour constituencies. People who have aspirations and don't want to be held back.
While this wasn't previously the case, the spatial and socioeconomic patterns are increasingly similar to that of the Democrat/Republican voters in the US, from what I can tell. The leftward travel of the Democrats is a large part of that. But the left/right inversion in the UK has been slowly coming for decades, but the FPTP system hid that in the outcomes.
Agree. As I once had it explained to me, "I don't choose parties any more, I just use my best guess as to which one will mean I take home more of my salary".
There's also the European angle. Those who want to work likely faced competition from EU workers and generally feel hard done by when it comes to globalisation. After all, if you worked in coal, steel, car manufacturing or your family did, quite likely you, or a relative, has lost a good portion of that work to cheaper manufacturing abroad. Which is more appealing: Labour, who prevaricated on Brexit, or BoJo, who simply said he'd do it? It isn't all that different to 'America First' in its appeal.
There probably wasn't any way to avoid the demise of coal, especially given our need to combat climate change, but did Labour provide an alternative? During the 2000s, Labour massively expanded higher education but also increased 'student debt', and only paid lip service to apprenticeships. If you're working class and working/aspirational, likely your budgeting is quite strict. Things like 'debt' and 'loans' generally mean 'trouble' and not a solution.
I agree this is broad strokes, but Labour has a problem in that it no longer actually represents its traditional demographic.
I think the idea that working people were feeling the heat from eastern european competition is a bit simplistic. Most industries have been facing a 'skills shortage', so people are generally aware that the health of their companies, and therefore their job security and career progression, are essentially limited by the pool of skilled labour. That and, working side-by-side with people from all over europe, people tend to feel a great deal of affinity.
The typical profile of a brexiteer is somebody retired, not somebody in employment, and I think the reasons are largely ideological, rather than practical; polling showed people who supported brexit would still do so if the hypothetical included economic pain.
It is a little bit simplistic, of course, but any such statement will be.
That said, I stand by what I said. If you look at maps of brexit voting tendency, you'll see they map quite heavily onto rural communities and former industrial heartlands. My explanation for this is that they don't see or feel the benefits of the EU and globalisation. But we didn't have a referendum on who wants globalisation to end, we had one on the EU, and so they took what they could.
> The typical profile of a brexiteer is somebody retired, not somebody in employment
I find this slightly weird stated so definitively having just argued I was being simplistic. I'll lay my cards on the table. I'm British but took advantage of free movement, so I've been party to more conversations on brexit than I really care to think about both back in the UK and here. Trust me, however, this is not an accurate statement: there are plenty of people with jobs who voted for brexit and have strong opinions on it. You don't need to take my anecdata on it though, we can look at a study https://yougov.co.uk/topics/politics/articles-reports/2016/0... - to put this into words:
- of every 100 18-24 year olds who voted, 29 of them voted leave.
- of every 100 25-49 year olds you meet, 46 of them will be leave voters.
- of every 100 people retirement age or above 36 in 100 you meet will have voted remain.
I find the 25-49 year old bracket overly broad, personally. The vote flips at 50+, but I suspect it would flip slightly younger based on my own experience.
But either way, it can't categorically be stated that all brexiteers are retired people. Actually I can lay further cards on the table: I used to do statistics as a job. So I take issue with the phrase "older people with fewer qualifications most likely to have voted brexit" used on the table I am quoting. Older people yes, but age also correlates with access to education, since my grandparents left school at 15, so there's a significant confounding factor here. I'd be interested in a more detailed breakdown, and I find the "and uneducated" part to be problematic/needing more evidence.
To come back to my point, I was offering a very qualitative interpretation of an extra factor I think encouraged previously core labour voters (in places that have returned labour MPs for about as long as there has been a labour party to choose) to switch allegiances in 2019. I agree with the fact labour does not represent them any longer. Brexit is part of, but not all of, that: I'm adding that Labour had an unclear stance on brexit, whereas these regions tended to vote more strongly for brexit.
This is obviously my opinion only, offered without guarantee or warranty.
I know this is brushed off or denied by the intelligentsia, and I know the ruling class (no matter what the party) never worked for the interests of the people but themselves, but nevertheless the working class is turning to conservative politics. The really sad thing is very few people on the left seem to be honestly asking why. What is their party doing so wrong that the least advantaged working class is voting for the parties traditionally associated with capital? Instead they seem happy making up feel-good stories about "the horrible uneducated racists voting against their own interest" to tell one another, and that is about the extent of their intellectual curiosity on the matter.
The right has no identity right now, which is why someone like Trump could take it over.
Depending on what happens in the next few years it could well be that they become the party against power. Which would be a rather interesting inversion from the last 40 years.
Which raises a lot of uncomfortable questions for people whose world was informed by Reagan, Thatcher and Bush.
Indeed. A lot seem to have lost the urgency of meaningful reform, because they don't believe it can be. They are out of ideas and unable to build the momentum to get anything passed. But they already have theirs, so ...
The biggest (and, rather oddly, rarely discussed) problem for the left in the UK is actually Scotland. Before the SNP rose to power, Scotland used to be a Labour stronghold. In 1997, Tony Blair's Labour had 56 seats in Scotland. Today, Labour have just 1.
Now that all of those votes go to the SNP it makes it extremely difficult for Labour to get a majority in the Commons along traditional ideological lines. There just aren't enough swing seats elsewhere to really make up for it. 200 seats haven't changed hands since WW2.
Seats gained/lost by winning party in elections since 1966:
1966: Labour Win, 47
1970: Conservative Win: 77
1974: Labour Win: 14
1979: Conservative Win: 62
1983: Conservative Win: 58
1987: Conservative Win: -21
1992: Conservative Win: -40
1997: Labour Win: 145
2001: Labour Win: -6
2005: Labour Win: -48
2010: Conservative Win: 96
2015: Conservative Win: 24
2017: Conservative Win: -13
2019: Conservative Win: 48
Current Seat Breakdown:
Conservative: 357
Labour: 200
SNP: 44
Lib Dem: 14
Plaid Cymru: 3
Alba: 2
Green Party: 1
NI parties: 18 (never been held by Labour or Conservative as far as I'm aware)
Speaker: 1 (politically neutral so irrelevant)
If SNP and Alba (Scottish Parties) are taken out of the equation entirely the way Northern Ireland currently is, Labour has only 18 seats that aren't held by Tories that they could potentially win. 326 seats are needed for a majority. That means Labour, in a best case (and very unrealistic) scenario where they gain all the seats from the minority parties, would need to gain 126 seats, with 108 of them coming from Tory seats in order to form a majority government.
I don't have the data going back past 1966 but looking at what we do have, a seat gain of more than 100 has only happened once: Tony Blair's 1997 win with 145 seats gained. 7 of those gained seats were in Scotland but Labour already held 49. In 1997, Scotland had 72 Westminster MPs but today, due to the redrawing of boundaries, it now only has 59. In total, Labour had 56 seats in Scotland. This means Labour held 78% of Scottish seats, which would equate to 46 seats today.
This is the real reason why Labour has had to become more and more Tory. To make up the deficit they either need to win back seats from the completely dominant Scottish National Party or win Conservative strongholds. They see the latter as more realistic so it's become their focus. When Scotland's seats are essentially out of reach of Labour, the UK becomes a de facto 1 party Conservative state.
It is absolutely bizarre to me that Labour won't make proportional representation and cross party co-operation a key part of their platform. Unless there are some seriously major shifts I can only really see Labour gaining power again through a minority/coalition government. Even if another right wing party such as the Brexit party emerged to splinter votes from the tories, Labour is still looking at a minority government. They simply can't gain enough seats unless they win back Scotland. This is why they are so reluctant to engage with the SNP because if Scotland really does leave the union, Labour probably won't be seeing power again unless there's electoral reform, a revolution or the tories mess up something up so badly that literally millions die. But by that point, they will have probably been in power so long (and absolute power corrupts absolutely) that they'll have the elections rigged autocracy style so even that may not matter.
That's what lots of people want - I can assure you, I know quite a few - but the British left attacks anyone so viciously and nastily that they aren't ever going to admit it to anyone seen in the vicinity of a Guardian.
The NHS has collapsed since COVID. No, it isn't due to lack of funding, that's a lie. NHS funding has increased massively under the Conservatives who haven't talked about even limited privatisation for the last decade or more. The reason it collapsed is that rigid commands and control systems cannot cope with change and the NHS was already dysfunctional before that. When they emptied the hospitals they created a massive backlog that they already knew they could never catch up on even with more funding.
At any rate it's irrelevant. The excess deaths are much more likely to be vaccine linked despite the collapsed state of the NHS. The timing, causes of death and split between vaxxed and unvaxxed doesn't really work for the theory it's lockdown caused.
NHS funding has increased massively under the Conservatives
That is simply not true. The Conservatives came to power in 2010. Here's what the The King's Fund [1] has to say on funding:
"In the decade following the global financial crisis in 2008, the health service faced the most prolonged spending squeeze in its history: between 2009/10 and 2018/19 health spending increased by an average of just 1.5% per year in real terms, compared to a long-term average increase of 3.6 per cent per year. These pressures were not unique to the UK, whose public spending on health care as a share of GDP is above the EU average, though lower than several comparable nations, including Germany, France, Denmark and the Netherlands." (Source: https://www.kingsfund.org.uk/projects/positions/nhs-funding)
[1] The The King's Fund is an independent charitable organisation working to improve health and care in England.
To put that 1.5% annual real-terms budget increase into context:
In the same decade the proportion of people aged 65+ increased from 16% to 22%ish of the population, an increase of a third. Since these are the people who consume the vast majority of NHS resource, the actual age-adjusted funding has been shrinking steadily every year.
But we're not talking about whether budgets increased by as much as random HN commenters feel would be ideal, I said funding had increased massively i.e. in absolute terms, which it has.
Any discussion of the NHS budget has to accept this reality - the British state is already deep in deficit for decades and had built up incredible debts just trying to keep the NHS budget rising, which it always has. To say the NHS would works better with more money is simply to admit it's broken and can't be fixed, because the government can't even afford the current levels. Especially not after the attempts to stop COVID blew debt and inflation through the roof.
We were talking about the NHS being underfunded, and you said that funding has increased in absolute terms. Both of these things can be true simultaneously.
But, we were not. This thread starts with the claim that "NHS funding has massively increased under the Conservatives" (true) and someone else saying "that's simply not true". But it is true.
NHS apologists always seem to try this switcheroo: someone will point out NHS funding has massively increased - an objectively true claim - and then they'll be accused of lying, by someone who claims it's "underfunded", an entirely subjective and different claim. As you point out, both can be true, but the latter is not disproof of the former nor even a well defined statement.
Looking up in the thread, I see "Another is the massive. underfunding of the NHS over the last decade" in the first post and things like "No, it isn't due to lack of funding, that's a lie" in the replies.
That definitely sounds like the thread was talking about underfunding/lack of funding to me.
Also, for what it's worth, I think your use of "massively" carries an implication to the reader that funding has increased above and beyond maintenance levels (i.e. that it's gone up in real terms, compared to inflation and demographic changes), as I think most people wouldn't describe increases that are below the level needed to maintain service relative to costs as being "massive increases". You'd probably get less pushback if you described it as "increased in absolute terms", or specifically pointed out that the funding increases have been lower than the underlying cost increases.
I know you did eventually add the "in absolute terms" part, but perhaps consider starting with that next time.
"I think your use of massively carries an implication to the reader that funding has increased above and beyond maintenance levels"
The word massive here just means a massive amount of money relative to other levels of government spending changes. From 2010-2020 most govt departments got budgets that went down (austerity), but the NHS was excluded and its funding continued to increase. The amount of money it got is truly massive even on the scale of government.
Trying to talk about "real terms" or "maintenance levels" with something like the NHS is impossible because demand for healthcare constantly increases even with a stable population demographic (some speculate that healthcare demand is actually infinite), as does demand for increased wages. History has shown that there is simply no level of funding increase that the NHS's supporters would ever consider sufficient because they can always claim that the system is strained, could use more people, better paid people, the latest treatments etc. So there's no fixed level that can be identified as maintenance, as one person's maintenance is another's underfunding, which is why all claims about underfunding are impossible to argue with - the statement is literally meaningless.
Related problem: enormous sums of money get allocated to it at a time when every other service gets cuts, explicitly earmarked for upgrades to capacity or buildings and it all gets immediately spent on pay rises in blatant defiance of direct government instructions. So service capacity doesn't change at all but govt can't do anything because too many voters worship the NHS and assume it's perfect except for lack of money.
You realise that this quote supports what I just said, right? It takes massive funding increases to consistently increase budgets year over year for over a decade by that much after inflation adjustment given how huge the NHS budget already is. Go on, compare the budgets between those periods in actual pound sterling terms and then think about how much more tax had to be raised to sustain that (or rather how much debt had to be issued).
They die of old age instead? Not really better. The point of the NHS is to treat people, if you have to wait three years for treatment that's the same thing as collapse, it's not really different from the user's perspective.
I'm genuinely interested in the link to the data about the vaxx / unvaxxed split.
I know the most ardent antivaxxers are going to explain every death in the next 30 years by the vaxx ; but the numbers would be so staggering that I suspect plain old counting would help.
Traveling today so don't have easy access to my bookmarks with that data (is heavily buried in UK govt websites) but here's an analysis of the excess death data that also shows ambulance call outs jump permanently and significantly in April 2021
A lot of it is due cardiac reasons. You can also look at when excess death went up in younger age ranges that weren't affected by COVID and see that it starts at the same time the vaccine programme reached them. Hard to explain as lockdowns given they'd been happening for a year by that time.
Edit: Here we go. here's an analysis of deaths by vaccine status for the UK:
N.b. The way you calculate the population size heavily affects the meaning of this data and the government itself doesn't know what the population is, so there's plenty to debate here, but you can see why the author concludes there should be an investigation. He uses a conservative pop estimate based on official NHS registrations (because the ons estimate is definitely wrong) and plots the graph of the difference by status at the end. So you can set that for everyone under 75 the vaccines appear to be making things worse not better.
I don't wish to be snarky, but you are aware that the NHS as an institution has existed since the late 1940's and has been working reasonably well for a long time? An institution does not become beloved by the public for failing to provide a good standard of care for a long enough time that people become used to it doing so.
So when you say:
> It never had a great track record to begin with.
Are you talking about government institutions in general or the NHS? I maybe wrong, but I suspect you're speaking of US institutions which are an entirely different dynamic to UK and European ones.
If you are speaking of the NHS, then please outline how it doesn't have a great track record commensurate with its lifespan.
>An institution does not become beloved by the public for failing to provide a good standard of care for a long enough time that people become used to it doing so.
Here's how you do it: you pump unsustainable amounts of money into the service over time. This allows you to offer a great service until in the future you can't pump enough money into it anymore. But that's a problem for the future generations. Those future generations were funding the previous generations all the while, but won't get the same benefits themselves.
An ever increasing percentage of GDP is being poured into the UK's NHS. At some point it's going to be too costly and the young generation at that time will have to pay for it, but won't get the same level of service themselves when they're older. They will be the ones left holding the bag.
I don't think there's a politically viable solution to this though. The problem with this model is that you're effectively borrowing from future generations, but the system takes so long to reach actual unsustainability that people will grow up with the feeling that the system is great.
Is £2,647 per adult per year an unsustainable amount? How much is is OK to spend on the military? On roads? On tax breaks for energy companies?
Don't forget healthcare isn't about you, it is about society and if you don't care about society just think of it instead as having healthy employees and customers, who aren't ruined if they fall ill, and therefore have cash to spend...
What's a better system then? Because it certainly isn't privatization. And correct me if I'm wrong, but I'm assuming that's what you're arguing for.
>you pump unsustainable amounts of money into the service over time. This allows you to offer a great service until in the future you can't pump enough money into it anymore.
This is how every growth based juggernaut business works as well. Quality of service always goes down to continue growth of profits, especially after you've crushed the competition.
IMO, healthcare of the public should not be a profitable business. Or the business will always find ways to squeeze their customers who simply need care for the health.
It's not so much the profit that matters, in principle. But profitability does provide some constraint and guide to resource allocation that a public institution is still grappling with how best to do. Private institutions can go under and be replaced more easily. Again, not perfect, but you never see the same creative destruction in government institutions.
I think general survey results are probably a poor metric to use in evaluating the success of a healthcare institution. Sure, at any point in time, most people should be able to get what they need, but the serious cases, or anything out of the ordinary, is a much smaller percentage of cases for any given year. Anecdotes of waiting lists and the rationing of care (e.g. delaying services to the start of the next fiscal year when new money gets distributed) have been notorious for years now. This dissatisfaction only reveals itself over time, where it personally affects a greater swathe of the people. The pandemic accerlated this, but it shows how ultimately unsustainable it is.
Healhchare is tricky, because treatments are not one-size-fits-all. Large institutions are rigidly setup to deliver a product, a product that is ever changing, as new treatments are always being refined and added. When it was created it was set up to deliver products that were new 50 years ago, but the structure is inherently slow to evolve. But the private health insurance in UK does not have these problems. More effort could be made at growing the economy in such a way that rising incomes allow people to purchase the private health insurance. It's not an immediate answer for many, but it definitely beats throwing more money at a bureaucracy that cannot adapt.
Isn't it possible that demographics have changed enough that funding requirements have changed enough that the 1940s-2000 or so system is no longer viable?
I know the demographics in the US has vastly changed some cost models over that time, making some earlier social program hit major funding problems through no evil from govt actors.
The demographics have changed, but they take that into account in terms of how they handle and manage care.
There's a lot of thinking and work that goes on to cover working out the changing needs of your population that has to be handled by any well managed healthcare service.
In the NHS specifically I am aware that they also have change management procedures that exist to try and understand how to provide continuous improvement as needs and situation change.
That's not to say things are perfect, by any stretch of the imagination. For example the NHS still has a big blindspot when it comes to tech. Most people aren't willing to take the effective pay-cut of being a techie and working in the NHS, a lot of people inside the service don't really respect people with tech skills and there's still a bit of a holdover of not paying much for anyone that isn't a doctor.
That's not to say the situation remains static, some doctors for example are slowly accumulating tech skills as a result, so what will probably happen is that success for a tech person in the NHS is going to require a prerequisite medical degree, at least in the near term.
Which though I don't think it's the best strategy, I can't also argue it's a terrible one to expect people who provide tech services into the NHS have a reasonably high level of domain knowledge.
This is a large institution with a substantial mandate, we should expect to pay a reasonable amount proportional to what it provides us. The fact that it's substantially cheaper than other healthcare services while still providing a very high quality of care leads me to believe that it's doing a pretty good job meeting that mandate.
So I don't think blindly questioning it without taking such things into account is helpful, nor do I think that pointing to costs as being "too high" are helpful without considering what is happening and why they are being paid for in the first place. Chesterton's fence and all that, it's not enough to just cut costs, you have to ask what doing so gains you. There are too many social programs which we cut because "spending less is good" without asking if the spending actually gives us a positive return as a society.
One common complaint from doctors (at least, in the U.S.) is the need to hover over a laptop all the time that takes time away from talking to the patient. A big problem as I've heard of a number of doctors retiring early because they don't feel as though they are even treating patients anymore, they are slaves to a console. (And these are not old doctors nearing retirement anyway.)
Personally, I think we've become a little too tech obsessed in thinking every problem can be solved with IT. Digitizing records only feeds a surveillance state anyway and can be dangerous (for other, obvious, reasons).
Well, doctors are mainly hovering over a laptop to justify their treatment plan to insurance companies anyway. They were not implemented because someone thought they would improve quality of care.
They have actively worked at crippling it. Now that it’s crippled they tell you.. oh but surely the government can’t fix it, we need private enterprises to fix it!
You walked right into it.
What makes you think private business are capable of delivering something cheaper than what the government can do? The most expensive health care in the world is private.
To be honest I'd be ok with private healthcare if they had to also obey the same constraints as public healthcare.
IE they had to provide care to everyone at a reasonable price.
I'm deeply suspicious of healthcare that gets to exclude people for cost reasons.
I too can provide great healthcare if everyone is mandated to pay me for my services and I get to exclude those I treat, that's a great business, the healthy pay and I exclude the sick, what wonderful pure profit business!
The insurance model bothers me for that reason, they really shouldn't be allowed to exclude anyone, if they're taking on the business of healthcare, then that's that, they are providing a utility service, which means they supply to everyone and they make money by spreading the cost between everyone.
There are nuances to that, but practically that's the goal they should aspire to, but unfortunately that model isn't the most profitable.
I mean take a look at the original US health insurance that existed:
> The first plan guaranteed teachers 21 days of hospital care for $6 a year, and was later extended to other employee groups in Dallas, and then nationally
[0]
That insurance model worked, it just happened to get outcompeted by entities who were willing to undercut them by aiming to capture only the most healthy people, which is in effect a tragedy of the commons.
Which is a real problem in my book, I'd be fascinated to see what innovations a private company could come up with under that model. We might have missed out on a whole slew of interesting ideas if we kept going down that route, which would still have been a pretty profitable business and would have been a great success for those who do believe that the private space can do healthcare better.
As it stands I don't believe the current private model meets that criteria as it fails at the first hurdle of being a health care service, it doesn't care about health.
So it seems like the choices are bad private care, good public care and bad public care. So yea, I'm leaning to the good public care.
Exactly. Why would it be cheaper or better to run healthcare as a for-profit business? If you have to take a profit, then by definition there's less funds available for the actual service.
The point of private enterprise is it has to cost less or be a better product to survive, which is why things like cars are unbelievably better than they were 50 years ago, or even 10 years ago.
E.g. saying a state-run car company would've done better because all that profit money would've been perfectly allocated is not right. Otherwise the government's perfect decision-makers would be starting car companies left and right and making a fortune, instead of working for the government.
Only if there is both competition and consumers can make informed judgements on the service.
In things that affect your health, I don't want to be the guinea pig that discovers the service I paid for wasn't up to standard. That provider may go bust in the long run, but in the meantime will do a lot of damage.
If fossil fueled cars burning leaded fuel on state funded roads and then getting bailed out not that long ago is your idea of free enterprise triumphing over the state, you might not be as capitalist as you think you are.
"Bob Lutz compares Tesla to socialism after GM took $11B from taxpayers under his reign"
I agree that cars are much better than they were 10 years ago. Thanks mostly to government regulations that the incumbent industry fought strongly, while Chinese state owned firms were taking advantage of the opportunity.
Roads aren't cars? I'm not saying that central planning is never a good idea, just that it's mostly not a good idea. "Where to put roads that a private company will build" is a reasonable role of government in a capitalist society.
> and then getting bailed out
I don't think they should've been bailed out. That was politicians buying car worker votes by doing politician things, like inflating the currency to make everyone's wages worth less.
Cars are better not mostly because of regulations, but because of manufacturing improvements, electronic/chip hardware and software improvements, and, most of all, competition.
This makes me wonder… if Conservative strategy is to run it into the ground and then privatise, which is an unpopular plan with the public, then how are they able to consistently win elections?
Largely because the Tories are also willing to be fairly openly xenophobic, which is very popular with a large portion of the public. "Making sure the poors don't take more than they deserve" is another one of their popular policies.
The more-well-off also think Tory policies will get them a house and security. In practice, the UK housing market is completely fucked and gets more so every year, but... it doesn't stop people believing it.
Basically the health of the NHS is about the tenth thing on some people's minds when voting, until they get cancer or break an arm, at which point they start complaining about it.
It is more nuanced than that. The issue is that a lot of western societies are falling into debt traps because of a lot of social and economic factors which are already straining these systems to the point that they cant keep up, and the conservative strategy (in my good faith interpretation) regarding this is reducing the cost of programs that they consider to be bloated. This can be interpreted as running it into the ground as the bloat is often in bureaucracy which can easily pass the buck to actual service providers which then suffer from lack of funding. In contrast a more liberal solution would likely involve increasing spending then trying to recover that through additional taxes, which conservatives would say doesn't solve the cost problem but rather exacerbates it since bloat remains and is paid for by more debt or taxes. Of course this is just a general simplification of the conflict.
Clearly the solution is probably somewhere in between, but political polarization has simply pushed people to their party lines and entrenched their positions such that no real progress can happen while things continue to fall apart.
NHS and Medicare have historically had both very efficient allocation of resources and excellent health outcomes. This NHS argument is about new data that to me seems impossible to deconflate with a global pandemic.
Basically, libertarians are just wrong on this. Government-run health care works great and we have many decades of evidence showing that.
This is the first time I have ever heard of Medicare being held up as efficient. Medicare is 13% of the US government budget. More federal money goes to Medicare than to the Department of Defense. In contrast, the care that people get from Medicare is substantially worse than what you get from private insurance in the US.
> Medicare is 13% of the US government budget. More federal money goes to Medicare than to the Department of Defense.
These are not measures of efficiency. Medicare outlays are about 30-40% of private insurance for the same demographics.
> the care that people get from Medicare is substantially worse than what you get from private insurance
And this is, in fact, not true at all. US citizens on medicare beat their cohorts not only vs. other nations but vs. private insurance in the US too. Don't make the mistake of comparing your corporate insurance for a workforce with a median age of 30 with what retirees in the private market have available.
There is no doubt that Medicare has the bargaining power to drive down hospital costs compared to private insurance: Medicare gets 10c/$1 on the chargemaster at hospitals (and hospitals set prices so that Medicare's payment rate has a small profit), while private insurance tends to be able to negotiate 15-20c/$1. Individuals who are good negotiators can reportedly end up paying only 20-30c/$1, so if you have a big hospital bill, it can pay to call them up and negotiate.
Retirees on the private market get completely shafted, though: almost everybody in their age group uses medicare, so the insurance will need very high premiums to cover their risks. From what I have heard, people who are on employer plans at that age have better health outcomes than retirees, regardless of where the retiree gets their healthcare.
> In contrast, the care that people get from Medicare is substantially worse than what you get from private insurance in the US.
I don’t think they are comparable. Medicare exists because private insurers refuse to cover old people at a reasonable price. It’s a good scam the private insurers have going: take peoples money when they are generally healthy and productive, drop them like a sack of shit onto the government’s lap when they aren’t.
The price of elder care in the US is not due to insurance companies, but due to the amount of attention someone demands before them die in a US hospital. Many socialized healthcare systems do not allow doctors to waste nearly as many resources this way.
That is why the life expectancy of the average obese, unhealthy American is about the same as the life expectancy of the average (much healthier) Japanese or European person. Americans are allowed to eat their way to an early grave and then have medical resources thrown at them to desperately keep them alive a few days longer.
EDIT: Also, I should point out that doctors generally demand a lot less end-of-life care than members of the general US population. They seem to understand that it is merely prolonging the inevitable rather than helping.
Funding, staff shortages and Brexit don't seem to get a mention in the article. The Government blames the NHS for the problems, but the NHS has no control over its funding. Tory idealogues are determined to increase privatisation, regardless of value for money.
We are never going to get a serious debate around reforming the NHS until people move on from only comparing the UK to the US. There are many other systems that work - people only need to look across to Europe.
In fact, I would argue that for all its possible faults (which all systems have) the fundamental problem with the NHS is not in how it is structured or in its processes.
Rather, it boils down to funding. Nothing else. Just that. The one feature that the NHS has proven time and time again is that it is one of the most cost-efficient healthcare systems in the World, and given that it is working suboptimally that is a clear sign that the NHS needs a significantly greater (and stable and dependable in the long-term) financial investment.
Once that is sorted, all other further changes and optimisations that may be needed can be worked on. But debating how the NHS needs to be reformed today is arguing on the helm of the Titanic on how to improve its unsinkability while it sails merrily towards an iceberg.
NHS funding increases constantly over time, often by massive amounts. The NHS is currently not merely suboptimal. You could have argued that before Team Expert came along in 2020 but not now. It's totally collapsed. There are now people routinely dying whilst waiting to be seen in A&E let alone the massive backlog for cancer. By any metric the NHS in 2022 has completely ceased to function properly.
There seem to be a lot of British people in denial of this fact. The NHS is dead. The only reason it still exists at all is because it isn't a company so the usual safety systems like bankruptcy can't force a reset.
Note that other countries which spend comparable amounts don't have this problem. I'm lucky enough to have left the UK a long time ago and lines in a party of Europe where the healthcare system is easy more privatised and less controlled by the government. Things here are normal, good even and I can get seen by a gp or specialist more or less immediately.
Still, merely "more vs. less" privatisation is not the determinant factor. Case in point, I currently live in Spain where universal healthcare is fully public as is the NHS(*), and over time decentralised and became fully devolved to each of the 17 autonomous communities (almost federal states in all but technicalities).
In general, from a user's perspective, Spanish healthcare tends to work better than the NHS in many regards, albeit with less flexibility at the GP level and more of a hassle when moving between regions. Anecdotally, from the experience of Spanish friends having lived in countries with a more or less public-private model (Belgium, Germany, Ireland) have expressed that the systems there are generally worse, and miss the Spanish healthcare system.
However, different regional governmens have made a greater or lesser move towards covert privatisation via externalisation, and while the two that have done it the most (Catalonia and Madrid) are generally the worst performers, there is little correlation otherwise. The Basque Country, Navarre, Asturias and Aragon are all top performers, yet the first two have privatised significantly while the latter two have kept the system more fully public. On the other hand, Andalusia with very little privatisation is together with Madrid and Catalonia as one of the worse.
And yet, when compared by investment, the pattern becomes much more clear. Madrid, Catalonia and Andalusia have some of the lowest healthcare investment per capita. The Basque Country, Navarre, Asturias are some of the greatest investers—Aragon not so much, but still on the top end of the scale.
(*) As a digression, due to historical differences in how each system evolved, they are not quite the same. Spanish healthcare evolved from Social Security, and thus used to require being either employed, officially on unemployment, or being a dependant of someone in either circumstance (now it's more lenient). Also, all doctors involved are state employees. The NHS on the other hand evolved as a right of all legal residents of the UK, and GPs surgeries are almost always private businesses that are adscribed to the NHS.
Look at g7 health funding by gdp for the last 40 years. The U.K. has been 10% lower than the rest (and about 1/3 - 1/2 of the US) for 40 years, Tory, labour, coalition, doesn’t matter.
That makes sense - we should find if there are any limits to the existing system after spending is increased to match Western European nations (~11% of GDP [0]). (my gut instinct says that we have hit those limits: if the NHS was a good model, you would expect another country to copy it)
If the healthcare outcomes don't resemble what other systems can provide with the same level of funding, there needs to be a serious discussion as to whether the NHS model is fit for purpose for today.
We (France) like to compare our sécurité sociale to the NHS, but only to remember that ours is not so bad after all. It’s never been the subject of serious debates, and the USA even less (rightfully).
> It's the EU that arguably needs to come back to earth, by returning to a trading bloc, rather than a halfway house pan-european state.
This old chestnut. Go read the Rome treaty or the Schuman declaration. The “it’s only economic” is a lie you’ve been sold by your own governments. The aim has always been political Union, from the beginning.
Besides, the EU being “a trading bloc” would not solve any of the issues facing the British government, which mostly result from the government having mutually exclusive demands and being unwilling to keep its word and following the agreements it signed. Including on imports and exports, which is the essence of a trading bloc and would not be improved one bit of the EU were only one of those.
> This old chestnut. Go read the Rome treaty or the Schuman declaration. The “it’s only economic” is a lie you’ve been sold by your own governments. The aim has always been political Union, from the beginning.
That's not true.
The Schuman declaration refers to the European Coal and Steel Community, which was about making war between countries materially impossible ie. through economic, not political, integration. It doesn't refer to stopping war by creating a common European Parliament with the idea that French and Germans should be subsumed into a European citzenry, with freedom of movement.
Similarly, the Rome treaty established the European Economic Community. The idea of European citzenship being only established with Maastricht as late as 1992.
The history of the European Union has been that of economic integration, with political union coming afterwards. There are many who would have preferred it not come afterwards. To characterise the project soley in terms of those who wanted a pan-European political project is misleading.
Political union has not really worked. The European Parliament is a weak institution, and the sovereign debt crisis showed how unpleasant the democratic deficit is, in this case for everyday Greek citizens, as the European Commission forced through austerity measures, triggering a humanitarian crisis.
> Including on imports and exports, which is the essence of a trading bloc and would not be improved one bit of the EU were only one of those.
The red line for the UK government is freedom of movement. If the EU remained someething akin to ASEAN, ie. prior to Maastricht, the UK would rejoin, and everyone would enjoy sensible trading amongst similarly economically developed countries again.
The EU's dream of German and Greek citizens voting together as "EU citizens" in powerful European Parliament on fiscal issues such as a shared pension age and sharing taxes, will never happen, so we have to wait until that folly is over and peoples using the Euro will continue to find out that they have ceded their democracies to undemocratic institutions.
> The Schuman declaration refers to the European Coal and Steel Community, which was about making war between countries materially impossible ie. through economic, not political, integration.
Right, I’ll quote it here for you:
“The contribution which an organized and living Europe can bring to civilization is indispensable to the maintenance of peaceful relations. In taking upon herself for more than 20 years the role of champion of a united Europe, France has always had as her essential aim the service of peace. A united Europe was not achieved and we had war.
Europe will not be made all at once, or according to a single plan. It will be built through concrete achievements which first create a de facto solidarity. The coming together of the nations of Europe requires the elimination of the age-old opposition of France and Germany. Any action taken must in the first place concern these two countries.
With this aim in view, the French Government proposes that action be taken immediately on one limited but decisive point.”
The CECA was from the begining the first step towards “a United Europe”, however close that unification might be. They just realised that they needed gradual steps. You can disagree with the steps, their size, and their frequency, but the end goal was explicit from the beginning.
> The red line for the UK government is freedom of movement.
And the common agriculture policy. And the fisheries policy. And the customs union. And the human rights. And Ireland. The British government had a lot of incompatible red lines from the beginning. This was obvious to anyone who has been paying attention.
> If the EU remained someething akin to ASEAN, ie. prior to Maastricht, the UK would rejoin, and everyone would enjoy sensible trading amongst similarly economically developed countries again.
That was a position (participation in the EEA but not the EU) the UK did not want to take. Besides, it was not even realistic in the first time. We are not in the 1980s anymore and Europe has changed quite a bit since then.
> The EU's dream of German and Greek citizens voting together as "EU citizens" in powerful European Parliament on fiscal issues such as a shared pension age and sharing taxes
That is not going to happen, at least in the foreseeable future, for several reasons. The first one being that the member states consider that their national sovereignty and they are the one pulling strings in the council. The Parliament cannot do that on its own, it’s just a convenient straw man.
> will never happen, so we have to wait until that folly is over and peoples using the Euro will continue to find out that they have ceded their democracies to undemocratic institutions.
More undemocratic than the Parliament in Westminster? You must be joking. And how accountable is the Bank of England? But yeah, rule Britannia.
Also, you forget that the British government pushed all the way along this drift towards a more neo-liberal, insulated from the whims of its populations, Europe.
> “The contribution which an organized and living Europe can bring to civilization is indispensable to the maintenance of peaceful relations. In taking upon herself for more than 20 years the role of champion of a united Europe, France has always had as her essential aim the service of peace. A united Europe was not achieved and we had war.
> Europe will not be made all at once, or according to a single plan. It will be built through concrete achievements which first create a de facto solidarity. The coming together of the nations of Europe requires the elimination of the age-old opposition of France and Germany. Any action taken must in the first place concern these two countries.
And as your quote shows, it's a long stretch to take the aspiration of a "united Europe" to mean inexorably leading to the problematic; often anti-democratic, institutions we have today. The aspirations were from the beginning economic, and there is no reason at all to think that this can instead take an intergovernmental, rather than supranational form. There was, contrary to what you suggest, no "single plan" that was always in place that governments have subsequently had to, in your words, "lie" about.
> And the common agriculture policy. And the fisheries policy. And the customs union. And the human rights. And Ireland. The British government had a lot of incompatible red lines from the beginning. This was obvious to anyone who has been paying attention.
No, it's freedom of movement, that's the main thing. There wouldn't have been Brexit without the European migrant crisis that shortly preceded it. Brexiters like Farage want a return to economic, not political, union, even if there is grumbling around certain policies.
> Be kind. Don't be snarky. Have curious conversation; don't cross-examine. Please don't fulminate. Please don't sneer, including at the rest of the community.
Comments should get more thoughtful and substantive, not less, as a topic gets more divisive.
Also please read Yanis Veroufakis's "Adults in the Room" on how the democratic deficit resulted in undemocratic austerity being forced upon Greece, resulting in a humanitarian crisis. There is no comparison between the ECB and Greece and the Bank of England and Parliament.
A return to a European Economic Community, with additional, optional, further integration around freedom of movement, for those who want it, would benefit the citizens of Europe. I don't expect that to happen, however.
No they shouldn't be looking europe. Modern healthcare is subsidization of chronically obese people by healthy working class. UK is the most obese country in western europe. Their situation is different cannot be solved by copying ideas from other healthy countries in europe.
I live in a US city with a metropolitan population of about 600,000. The largest provider in town is a university hospital with a sprawling set of clinics that employs 1850 physicians and 21,000 staff. I have pay for insurance that provides the best coverage in my area.
Last September I asked for an appointment with my GP before the end of the year. The first appointment was on January 3. I took the appointment. In October they called to reschedule that appointment. I could take a video appointment another time in early January or an in person visit in June. I took the virtual appointment. Rather than charging a $200 facility fee, they charged a $70 for the telecommunications that were pretty much the same as a zoom call. My insurance would have covered the room charge as required by law. They refused to pay the telecom charge.
Last December my GP ordered a routine screening procedure at my request. I was hoping to have that complete before my January visit so we could discuss any interesting results. In July the clinic that performs that procedure called to schedule the procedure which is scheduled to happen this week.
For this procedure, the clinic is requiring a negative Covid test. They scheduled this test at the one place that they provide these proactive tests. This is a drive through test site that is a 25 minute drive each way from my home. They provided an estimate of the costs for this test. That is $399, which (before taxes) would be earned in 23 hours by someone making the median wage in my city. My insurance company doesn’t think the Covid test is medically necessary so will not cover it. I canceled that Covid test appointment and got a free test at a more convenient location from public health.
Apparently they do this so that people aren't surprised at the magnitude of the bill. Last September I got a covid test at the same place as I had symptoms and was just about to travel. They didn't provide an estimate at that time, but looking at my insurance statement, I see they billed $394.35. The negotiated rate meant that the provider was paid $184.98.
Looking back at my past estimates, I see that in 2015 the estimate for the MRI ordered by an ENT that was diagnosing hearing loss was $11,427. In Canada, apparently a private MRI would cost $1,000 or less [1]. I bet the fact that they are available for free for those willing to wait a bit longer helps keep the cost down. If I was given the choice of paying $500 or waiting a few more months for free, I would have definitely taken the free option because I had already delayed care on this for over 10 years.
My wife works with people that are undergoing cancer treatment. One of them is single and lacks FU money in her bank account. She needs to carefully manage the 20 weeks of unpaid leave available to her (and a couple weeks of paid sick leave and vacation) so that she doesn't lose her job. While COBRA could provide continuation of benefits at her current level, that is quite expensive. The Affordable Care Act would give her a path to affordable insurance, but her recent salary would seem to put her out of the running for a full subsidy. Switching insurance in the midst of treatment could mean switching providers. Surely switching providers from one of the best in the area (which is open to Medicare) to someone else while in the midst of cancer treatment is not ideal.
Per the Canada MRI pricing, a private option can be an empowering alternative. A high-quality public option is needed to keep the private options in check and to provide a base level of care for those that are not lucky enough to be able to afford private insurance and private care. Even then, surely there are horror stories.
Indeed, transparent pricing is a plainly obvious requirement of a free market, which is why lots of business "innovations" are ways to hide pricing. Where it breaks down in my mind is that we have a hard time assigning a market value to human morbidity and mortality.
I have my own story of US healthcare which may be enlightening. It happened to a friend of mine. Let's say this friend is not particularly well to do and lived with his 2 brothers, but they don't always get along that well. At some point, they got into an argument that escalated into an altercation where one brother broke a poolstick over my buddy's head. He had a concussion and laceration needing stiches, so he went to the ER. He was unable to remember his name or which ER treated him, and as a result, was never billed for the care provided and learned the key to universal healthcare in the US - he just gives a fake name at the ER now.
One person I'm speaking to claims that the NHS hires too many bureaucrats who are impossible to fire, and who he believes provide the doctors with too much paperwork. He suggests that instead of paying those bureaucrats, the money should go to doctors, nurses and equipment. He claims that the NHS gets about the same amount of money - GDP-wise - as other European countries, while underperforming them. They already hire >1 million people out of a population of 70 million, and paying them more is unsustainable.
As someone who was embedded in the NHS for a number of years it has many problems, but counterintuitively one of them is actually a lack of paper pushers or at least low level admin and other auxiliary staff.
Because governments have constantly demanded the NHS spend less money, but have also been under pressure to preserve numbers of "front line" staff you've ended up with serious shortages of low level admins, medical secretaries, receptionists, finance officers etc. This means that more and more healthcare workers spend their time doing paperwork or customer service work that could be done by anyone. I worked out of one of the largest genomic diagnostic labs in the country with over 150 clinical geneticists, nurses, scientists and consultants and there were 4 admins. That meant nurses were staffing reception, consultants were managing their own diaries, geneticists were doing stock takes and clinical scientists were packaging up and booking samples onto DHL for collection. This was not an efficient way of working, but the lab had a hard ban on hiring any non "front line" staff. And it had been running like that for years.
The trust as a whole had the same problem on a macro scale. There weren't enough finance officers so invoices didn't get paid or debtors chased (the NHS provides a lot of private services as well). Because of a lack of staff working in recruitment it could take months (4 in my case) between being given a job offer and the paperwork being in place to actually start. Payroll was a nightmare because of lack of staff and multiple unintegrated time recording systems, many of them to this day paper based.
A large number of legacy patient records are still paper based and have to be physically moved around and digitised "on the fly" but because the NHS is supposed to be digital there aren't enough porters payed to literally push the trolleys of records around so you end up with nurses doing it.
I could go on for a long time but you get the idea.
The shift in the western world into paper pushing in healthcare, education, construction, etc doesn't always come in the form of more bureaucrats. Sometimes it's teachers spending time with ever more frequent and granular grading and survey systems, and doctors filling forms for hours a day.
It feels like the McKinsey-style design of large orgs has permeated the public sector just as much if not more than the private one. It always comes with a massive amount of procedure – employee surveys, follow-ups and meaningless 10-scale measurements, so that leadership can rest easy knowing that every decision they make is data driven. Somehow a spreadsheet analyst should be able to diagnose and fix every possible issue in an incremental manner, and conversely, all poor decisions are due to insufficient data.
Yes the demand to have a documented policy, procedure and metrics for everything even if no one ever reads them, follows them or analyses them is insane. At the same time there's been this huge increase in the amount of useless correspondence and a cultural shift away from hiring people to help manage and filter this stuff so people can do actual work (aka old school secretaries and admin assistants). Harrumph
Yes it SHOULD be. But the anxious leaders want more data for no other reason than to look at it and think they're more informed, when in reality they are not. It's like being addicted to looking in the mirror. It's good if you can notice the chocolate around your mouth, but more than that isn't helping, it's just a hobby. Only in this case your hobby is destroying everyone else's joy and productivity.
Lack of administrative staff in operations is a mayor problem, pushing paper work to medical staff. Where I live we have the same problem in schools, pushing administration to teachers.
Admin bloat seems to be at a higher level if it exists. Because ordinary secretaries are long gone.
On the other hand, my ex worked for the NHS. To 'solve' the problem of long wait times after check in. They reduced staff at check-in to bottle neck the in flow of checked in patients.
> This means that more and more healthcare workers spend their time doing paperwork or customer service work that could be done by anyone
The obvious solution seems to be reducing the required paperwork rather than hiring more staff to handle the paperwork, and this seems to agree with your experience when you described "unintegrated time recording systems".
That said, I wouldn't be surprised if too much bureaucracy was also partly to blame, because that's what happened here in Canada.
That sounds like exactly the kind of thing you'd say, if you wanted to destroy a beloved public institution though.
Most people are worried about the UK moving to a US model, not to be more like Norway, Netherlands and Australia and administrative efficiency is something the NHS does well:
> Conclusion: Four features distinguish top performing countries from the United States: 1) they provide for universal coverage and remove cost barriers; 2) they invest in primary care systems to ensure that high-value services are equitably available in all communities to all people; 3) they reduce administrative burdens that divert time, efforts, and spending from health improvement efforts; and 4) they invest in social services, especially for children and working-age adults.
I have relatives working in the NHS bureaucracy, even they claim its bloated - there's a fuck tonne of redundancy/duplication of effort and failures to exploit economies of scale, especially in the Trusts system where the same things are replicated dozens of times.
This sounds plausible, because it's a story we hear all over the world, again and again. I'm guessing David Graeber's "Bullshit Jobs" has been discussed a few times on Hacker News?
This was such a phenomenon in the seventies that by the time Yes Minister was broadcast the joke was a running ironic theme that met with deflated apathy:
Literally yesterday the Daily Mail published a front page ‘exposing’ the fact that the NHS spends a total of £1 million on diversity. If that’s the best a paper hellbent on attacking the NHS can find, it’s hard to imagine there’s actually much waste.
Regardless of private or public, left- or right-wing, bureaucracy begets more bureaucracy. Like a ratcheting effect.
Complaints about bureaucracy is (at least) as old as written history. You may have seen yesterday's frontpage story "The Collapse of Complex Societies (Book Review)" https://news.ycombinator.com/item?id=7207348
Another interesting analysis (for us geeks) is the "complexity catastrophe" described in the book Design Rules: The Power of Modularity. TLDR: Dependencies eventually get so tangled that the cost of change outweighes the expected benefit, and a system which can no longer adapt to the changing world eventually fails outright.
Exploding overhead also happened in education, both K-12 and higher ed. And probably every other mature domain worth examining, if we bothered to look.
Seeing Like a State (James Scott), Bullshit Jobs (David Graeber) and Design Rules (Baldwin, Clark) all address complexity in their own way.
As a geek, I think "path dependent technical debt". For us, there's little to no incentive to cleanup, and certainly no reward, even though everyone moans about it nonstop.
The only notion I have is that, like reducing technical debt, fighting admin overhead (expanding bureaucracy) requires constant effort and investment, that no one is willing to make.
I (greedily) welcome a more optimistic take on this problem, if any one has some ideas. Please.
That's because each of the several hundred billions of pounds of greenfield government software programmes is a slapdash crud forms exercise bugger the millions of man years of development by the original experts despite there's little to change in the vast majority of diagnostic pathways. In fact the Reed Codes which resulted from a immense pan European study of two decades length and became canon in ca 1988 remain canonical the only programming work involved in new processes being parsing these together with inserting a myriad of OR impedence where new forms of graft are inserted. We've just switched off national critical systems of civic function across the board over the past few years. Probate about the most egregious example the replacement system containing a mere handful out of the estimated twenty thousand expert legal assessment rules at inception. Manual operations the only alternative for at least two years that I was paying attention.
An aging obese population is the elephant in the room. This problem is not only happening in UK.
About 15 years ago the NHS tried to add easy to read labeling to foods with a semaphore: red, yellow, green. And it was blocked during a Labour government with majority.
Giving it more and more funds while not fixing the underlying problems is going to cause a massive budget crisis. We need to fix the causes not the symptoms.
"easy to read labeling to foods with a semaphore: red, yellow, green"
Easy to read, OK, but would it actually be reliable?
It is way too easy to label avocado red because of high fat content while labeling a candy bar orange because sugar isn't officially considered that dangerous ... and unlike avocado farmers, highly processed food producers have a good lobby.
> Even people who have experienced appalling treatment feel the need to exonerate the NHS when complaining about their experience.
It really depends on the context. Many will defend nhs because the alternative pushed from time to time is a privatised system which would only make things worse. I'm definitely in the "be careful how you criticise the nhs" camp. It's not great, but let's make sure Tories don't hear that as an encouragement to take it apart.
I’m not someone who thinks the setup of the NHS is untouchable, I currently use and prefer the Dutch system. But I’m not convinced the NHS needs changing as much as it needs proper funding.
Change alone would not make much of a difference. It’s definitely mainly a funding issue. But some change is necessary, particularly where the tech side is involved (lack of record sharing, old systems vulnerable to ransomeware attacks etc).
>Unfortunately without a change in government we’re not going to get those and people are seemingly more concerned about refugees arriving by dinghy than health care.
One can be concerned about both.
If we ever had a socially conservative and economically progressive government they would stay in power until they died. I mean in the US they literally had to add an amendment to make sure it didn't happen again: https://en.wikipedia.org/wiki/Twenty-second_Amendment_to_the...
I didn’t say that you couldn’t. But by voting for the current day Tory’s you are choosing to decimate the health system and waste money on sending Refugees to Rwanda. It’s idiotic to prioritise that over the NHS.
>> decimate the health system and waste money on sending Refugees to Rwanda. It’s idiotic to prioritise that over the NHS.
It all depends how you view the world. For many people, preserving the historical character and demographic of their country is an important issue. It might not be to you, you might consider it stupid, but it is a concern many people have. So much so, they would see illegal arrivals of non historical descent as a more acute problem. One to be prioritised over what can be argued to be improvements to the existing system.
I myself am one of these people. It is more important to me immigrants be sent to Rwanda than offering additional funding or reforming the NHS.
If my interaction with other people sharing your beliefs ( or more accurate my assumptions about your beliefs ), you believe me to be evil. I do not believe I am and I do not believe you, who think the opposite of me to be evil. I believe you are misguided though and wrong in what your priorities are.
Wait, I’m seriously confused by this. If preserving the character of one’s country is an important issue, is the NHS not part of the character of the UK? My understanding is the NHS is one of the defining symbols of the UK, a showing of communal strength and compassion, the Western sensibility in the face of the devastation of war. It touches everyone who lives there, is born there, and often when they die there. It’s erosion is changing every single citizen by shaking their faith in the underlying values the institution represents. Isn’t that a way bigger change?
Genuinely, why are refugees something to be prioritized over a cultural touchstone institution if the goal is preserving historical character?
Supporting the party which consistently underfunds a British institution, and sells off parts of it to their mates, in order to protect Britishness. Sums up Tory politics nicely, really.
From what I see, the British values seem absolutely normal to me, and healthcare results (life expectancy, 5-year survival of cancers) are just fine, especially given how fat British people have become.
"Funded enough" would mean things like GP appointments in days rather than weeks, and specialized diagnosis/treatment in weeks rather than years.
What percentage of GDP would be needed for that? That question would require a lot of data and analysis to answer, far more than would be reasonable to expect for an HN comment.
The problem is caused by the current in-power political party wanting to run the NHS into the ground so they can use the resulting bad performance to justify selling it off to their mates.
Very similar to Canada as well. Healthcare funding was limited before Covid (12-24 months wait for joint replacement), but with the 2 year hiatus on screening and non-urgent procedures, plus mass burnout of healthcare workers the system is close to imploding.
Now it's pretty routine to just go to urgent care since it's unlikely you have a family doctor, ever. Rural hospitals and clinics are either reducing hours or just outright closing due to lack of staff.
The difference is there is no private healthcare in Canada (there is, but it's minuscule).
You either wait for the public system or you fly to the US.
I met a guy in Vancouver who was flying to the US to pay $36,000 to get his knee replaced because his doctor told him "the wait was 2 years before Covid, now? it's indefinite". Guy was a highly active 65 year old and realized $36,000 was cheap if it meant he didn't have to give up 5 years of his best remaining years waiting for the Canadian healthcare system.
Quite a few OTC drugs in the US are prescription in many other countries. Antihistamines are another example of something that requires a prescription in some European countries.
Honestly - it should be, considering how people are absolutely ignorant about it's potency to kill the liver. Especially because some use it as a hangover painkiller.
Coincidentally, there have been a large increase in heart issues, and SAD (sudden adult death syndrome) happening too.
This appears to have started back at the end of 2020, in waves over the last few years. First, the elderly, then filtering down to the younger age brackets.
All in the wake of the terrible things you have mentioned.
Having worked with the NHS for years, I've seen the good and bad of it. The nurses are the rock, a lot of the doctors seem great, others quite alarmingly without common sense. The management seem to have a policy to "promote to incompetence", and the government intervention seems to encourage the wasting of the vast sums of money they are given.
It's a perfect storm, people don't want to recognise what is happening, the NHS is dead already.
> While the people that work there are not the problem
They are not responsible for the lack of funding but my experience with NHS's admin has been pretty bad and they can't blame "government's cuts" for everything.
I know people who work in consulting in the Big Four and everyone wants to avoid NHS projects because of their internal organisation and waybof working.
The NHS has a big organisation and quality of people problem as well.
It is a sacred cow, as you mention, and in general people are reluctant to say anything bad about it.
The Tory government are doing it on purpose to get the people to want to move to private healthcare. Amazingly it isn’t working, even tho they have basically destroyed the NHS. The silent resilience of British people has backfired on them. Truth is that many old Brits would literally rather die than kick up a fuss
The fact that the response to trashing the NHS from some sectors would be counterintuitively to insist on trashing the NHS more (as some kind of punishment I guess) is exactly what the people trashing the NHS were relying on in the first place.
"It takes forever to see a doctor on the NHS, now!"
"Let's get rid of the doctors altogether and see how they like it! They think they're so safe."
This thread really matches well with the thread about teacher shortages. The problem with the NHS is that it should cost far more, and should turn people down when they can't pay. Then patients would understand their place in relation to doctors, like in the US, and stop complaining.
> Another is the massive. underfunding of the NHS over the last decade. This has become much more evident post-covid thanks to the backlogs.
If this were the true issue, the excess deaths would have been starting at peak Covid hospitalization. In fact the opposite is true…
That said, particularly on any bureaucracy- more money doesn’t solve issues. In fact, more money often makes more bureaucracy. Obviously that’s not only the case, but it’s one I’d seriously consider here.
The historic squeeze in NHS funding has shown up in all sorts of metrics: most notably waiting list times - which have exploded over the last decade. Health prioritisation means the doctors can try to reduce the immediate deaths - the major costs being pushed into pain and suffering of people waiting for operations (but not dying, or being rushed in if they go downhill). All of this just kicks the can, and left the NHS at breaking point - ready for covid to break it.
On bureaucracy - a health service requires administration, so any health funding can be described as "more money for a bureaucracy". The evidence shows that I direct public service like the NHS - concentrating on building hospitals, hiring doctors and nurses and making people well - involves somewhat less administrative costs than using an indirect insurance system (like most European countries, Canada etc) and much less than the dysfunctional private system in America https://www.healthaffairs.org/doi/10.1377/hlthaff.2013.1327
I'm not convinced that the UK has been all that comparable to Germany and France for years. GDP is of course an imperfect measure of the real size and capacity of the economy - Ireland has about twice the GDP per capita of all of those countries, but there's not really any way for their government to capture that economic activity as funding for stuff - and certain other metrics are not so great. For example, the average UK household is apparently £8,800 a year worse off than in Germany or France (median income, adjusted for purchasing power) and that gap's been there since about 2008: https://www.theguardian.com/business/2022/jul/13/average-uk-...
In some sense, the UK became poorer than the other European countries it'd normally be compared to at the end of the previous New Labour government when the financial crisis hit and just never really recovered from that. It's possible there is no obvious way out anymore - everyone being poorer means less means less money for them to spend on consumer products and services and less tax revenue the government to spend on things like healthcare and infrastructure, and all of that means less businesses interested in setting up in the country (for reasons other than low taxes anyway) and less tax revenue, less well paying jobs... it's a vicious circle to be stuck in.
Even before that happened, the New Labour-era spending was obviously unsustainable at the level of tax they were willing to charge. Despite the economy booming and a bunch of NHS infrastructure spending being moved off government books via expensive PFI programs the national debt went up consistently as a proportion of GDP year after year. Afterwards the Tories made a big fancy show of austerity and cutting back on government spending (and to be fair it did eliminate the deficit like they promised, for a while anyway) but even their big scary austerity program only froze the proportion of GDP spent on healthcare for a while.
I feel like we always end up having the same debate.
On side says "Not enough money"
The other side says "But money don't solve problems, there's an effciency problem"
Both are true. Maybe we can now admit that yes bureaucracies are generally inefficient (by design. Why would seek efficiency when it can provide safe jobs for a part of your population that you can now get out of your unemployment stats)
and yes public healthcare system have been massively underfunded, probably for ideological reasons, in order to open up the market to private healthcare like European Union wants to open anything to market. (Look up what happened when they "opened up" the electricity market in France, what a joke)
I agree with almost everything you've written. The NHS is indeed treated like a sacred cow, and it is absolutely not world beating. I live in Switzerland, but am British, and I would infinitely prefer to get my medical care here and to pay for it. The French medical system has a better reputation than ours also.
Swiss medical insurance is actually quite strongly regulated and not like the US system at all. Extras are generally where insurance make money, like having a private room in a hospital instead of a ward.
Where I disagree is that a change of government will improve things, because I don't think 'more money' will magically solve all of the problems. As an example, GPs should be doing face to face appointments again as you say, and they should be on call for out of hours. Not for extra money, they're already highly paid. This is just part of the job - people aren't ill conveniently between 9-5 Mon-Fri. Before anyone says this is unfair, UK software engineer salaries look nothing like US ones most of the time, whereas doctors are 'raking it in'. Yes, being a doctor is a tough profession, undoubtedly, but getting into medical school is highly competitive and sought after. So you either want the status and money in exchange for unsocial hours and dealing with the sick and dying or you choose a different career.
I don't find it a convincing argument that 'this is all the fault of the tories' because I also had a problem with panic attacks when I lived in the UK under a labour government, and was also outright refused treatment because our local area had only adult facilities and I was 17.5 when it started. I've plenty of other stories, but this is mine.
Generally UK politics is polarised like the US and people who believe the conservatives' sole motive in life is to dance on the graves of the poor while watching a food bank burn are likely to be overrepresented online. Remember that austerity came on the heels of Gordon Brown trying to spend his way out of a recession, the same PM who as chancellor sold off the UK gold reserves at the bottom of gold value and tax raided a bunch of pensions. Labour are by no means perfect either, and unfortunately even governments have to budget.
Don't get me wrong, the tories have been the government for quite a while now. They've had time to improve things and they definitely haven't. I'm just saying the idea Labour will magically resolve NHS issues is a fallacy. I'd argue that the real issue is the short term/electoral driven policymaking with regards to the NHS - it is a sacred cow, and even the slightest mention of change could potentially be political suicide.
> Getting a GP to see you in person is now quite difficult (they want to do everything via phone)
Doesn't really strike me as a bad thing in itself.
Once you get past the front line, things get pretty specialist and a general move to Telemedicine is probably a good thing, and is presumably happening all around the world for all sorts of reasons. People even do telesurgery now.
And yeah, in a world where someone is continually lying about something good and useful, you do need to choose your words carefully to not help spread their lies. That's not anyone's fault but the liars though.
Preventive care is absolutely the most important to keep the society healthy and moving forward.
Currently people just give up on contacting their surgeries, letting their symptoms develop into something potentially more dangerous. Then they end up at A&E, overloading the hospitals.
Maybe it's not so bad in the 3 biggest cities (possibly due competing private services), but at smaller cities and towns, it's impossible to see your GP.
I see people complaining about it in pretty much every media.
The NHS spends a lot of money trying to get people to use the right level of care, like pharmacists, info on the web https://111.nhs.uk/ and by phone.
I don't particularly see a face-to-face visit to a GP when you think you have an issue as preventitive, but if it was, I still don't see how telemedecine wouldn't be a partial solution to that problem, not make it worse.
Right. I think the argument being made here is that if the job of the GP is just to route you to the appropriate specialist, well, they can do that virtually.
The word "funding" does not appear in this article. The NHS has been systematically underfunded since the Conservative entered power more than a decade ago. The crisis is real, but it is a political choice.
The pressure on NHS budgets is largely due to economic conditions. Looking at funding compared to GDP rather than nominal terms shows this. NHS funding peaked at 7.5% of GDP in 2010, but that peak was mainly due to a drop in GDP, not an increase in funding. With tax revenue declining due to recession and an extended period of low growth those funding levels were unsustainable. We're still actually spending about the same percentage of GDP on health care now as we were in 2009.
The blue bars in the chart are recessions, when funding relative to GDP jumped mainly due to a drop in GDP, not an increase in funding.
The historical lesson is yes, if you want big increases in NHS funding elect a Labour government (although by 1997 the Conservatives were already ramping up health care spending), but I'm not convinced the UK economy has much leeway to support spending a lot more than the current 7% of GDP on health care.
The UK has a similar system to Canada. Costs are controlled by controlling the funding. You set a cap to what you'll spend and let the system figure out how best to allocate those funds. It's a big reason why the cost per capita for healthcare is quite low - you simply choose not to spend more.
The demand for healthcare spending is almost infinite. You can set it up so everyone get an MRI the same day the doctor orders it. If you cut back and it takes a week for a non-urgent MRI is that a "proper" level of funding? How about waiting one month? Two months?
The truth is, a country needs to decide how much money they are willing to spend on healthcare. Some spend very little, some spend a lot. There is no "fully funded" system, only trade offs.
Unfortunately that's in line with the Bank of Canada's recommendation:
------------------------
"Mr. Macklem: [... T]he high inflation that we have today is not normal. It's not here to stay. We are resolute in our commitment to bring inflation down. We are taking action and we will continue to take action to bring inflation back down. So as a business, don't plan on the current rate of inflation staying. Don't build that into longer term contracts. Don't build that into wage contracts. It is going to take some time, but you can be confident that inflation will come down.
The reason he speaks to that is that he's worried about inflation increase due to a wage-price spiral. Depressing wages is a way to prevent that. And I'll mention now; I have no idea how true this is.
As a start, that means that your costs have substantially increased to provide the same amount of healthcare as before. That makes the funding problem bigger. I'm not sure how it is in Canada, but the NHS in the UK employs about 1.4 million people - and a lot of the problems with it are actually problems with our social care system being broken and leaving it nowhere to discharge patients to, which accounts for another 1.6 million workers. The UK's population is about 70 million people in total, a reasonable proportion of which are either too young or retired. This is only going to get more daunting as the population ages here and in other western countries, and as new treatments are developed and healthcare expectations increase.
On top of that, the real economy's capacity to supply workers with stuff to buy with their income is in deep trouble worldwide right now and everyone is feeling it. That means real wage drops across the board and real damage to the ability to actually fund something like this.
Generally it has nothing to do with money. What you actually need to decide as a nation is how many people will work in the healthcare service, rather than in the private sector producing stuff others consume.
Healthcare is an insurance service itself. It's designed to keep people going so they can continue to contribute to society.
The more productive the producing sector, the more of society you can have working in healthcare.
But let's ignore the blairite solution to sell the land and get further into debt and refuse to take more money from the populace or detach NHS funding from state pensions...
You would think that but a lot of people can't see beyond its the Tories in power. We'd be better off with proportional representation but the beeb did an excellent job at mis-selling that to the masses
It is frustrating to see the country getting polarised this way. A 2-party system is not helpful to a functioning democracy. I am not a fan of fully proportional representation as it leads to government instability and ineffectiveness, but a party getting an absolute majority in Parliament whilst getting 40% of the vote is a travesty. Also, after having lived through Brexit and the successive government, the BBC is not fit for purpose. It is fine as a public media group, but it’s sanctity in the mind of a lot of British people is not really well founded.
Yeah have to agree with pretty much all of that. My worry is that we are defecto the 52nd state these days and we've adopted the 2 party system from across the pond since the coalition was little more than a sitting government against fox hunting, their arguably biggest achievement was placing Cameron in a position where he bailed after throwing national policy under the bus to appease his own party.
I won't pretend that Brexit hasn't been mishandled as a lot of the opposition predicted (also in news water wet), but the EU/EC has unfortunately for them shown a lot of its attitude toward Britain is as promoters had been saying.
I'd argue that the UK has always had a 2-party system, and if anything the US adopted it from us. The Lab/Con split goes back to ~1910, prior to which we had the Tory/Liberal split going back to ~1850, prior to which we had a Tory/Whig split going back to ~1780, prior to which the political system was very different.
I'm not citing evidence for that I'm showing how both sides of the political divide won't dare touch the holy cow that is the NHS.
It's interesting how every time you show there's a problem with a political party everyone assumes instead of damning the system your trying to politically point score. I think the real change needs to be made in the civil service and certain powers striped from Whitehall but it'll never happen.
I'm not even making a moral judgement here. One of the key traits of right-wing politics is advocating the free market and private ownership. Privatising the NHS is not a left-wing policy.
In 1997 the NHS had 1/5th the budget it does today. Do we think that service has improved 5 times in the period?
Like universities the NHS has been eaten from the inside by administrators whose sole purpose is to keep doctors from doing actual work. Talk to a nurse and 4/5th of the bullshit they have to deal with is pointless paper work.
CPI over this period was about 80% but large % of NHS costs are salaries so would be expected to run ahead of CPI by at least 1%.
Net of all this funding has gone up by say 50%-100%
But over this period the UK has had a very large increase in the elderly population who are disproportionate users of the NHS (over 85s up by about 80% roughly I think).
Having had quite a bit of contact with the NHS over the last few years I’ve seen much less form filling than I’d probably have expected.
And of course that form filling for the nurse is also known as data collection / management information which in any other context would be deemed essential for proper management of the service.
This is misprescription - it's the LACK of administrative staff to do that specific paperwork that has caused this. Political microwaving of the whole system to "reduce costs" but keep "front line staff" has meant everyone is doing jobs they arent qualified to do and suck at.
The amount of people who think they understand the NHS is interesting, and clearly newspaper driven.
‘Too much management’ has long been a tabloid argument to restrict funding - see the Daily Mail front page yesterday.
There was a TV programme ‘Can Gerry Robinson save the NHS’ fifteen years ago that had some very interesting examples of problems with lack of effective management.
A systemic risk to national healthcare systems is that they can be underfunded (or overfunded) in a way that private healthcare can’t because individuals are more diverse and make decisions more attuned to their individual situation. People have different preferences for how and how much they would choose to invest own healthcare, and if everyone is forced to bear one another’s bills, there will inevitably be people who are unhappy with the group’s decisions. Since it’ll be a compromise of different groups, I can imagine it’d be destined to frustrate both sides 90% of the time.
Well yeah that's how every insurance works, including private ones. You are put in a pool together with others who may be more or less costly than you on average. Not just insurance either. If you're buying stuff at all you're paying a premium for stuff you're often not using, eg customer support, return policies, marketing etc.
One you accept that you never have identical cost/benefit with others, we're just talking what level is acceptable, and what services should be covered. People seem fine with paying for fire departments, even though some people live in wooden houses and have candles at night. Healthcare has a similarly low fraud incentive, and is generally not something we "invest" in. Most of the world has recognized that and arrange it through a publicly funded system.
It's still difficult for a lot of people to get a physical exam by their GP. My own mother had her breast cancer diagnosed pre-pandemic only after she came in with an unrelated problem. Many health problems are not being caught while GPs are working from home.
Related complaint: My mum was nearly deaf for six months. She got a few remote appointments with her GP surgery. One recommended she get psychotherapy. Another said she had a "foreign body" in her ear. After six months, she finally physically met a specialist who said she had too much earwax, and after vacuuming, she now hears better than she has for years.
My parents are dual citizens, so they'll be leaving so that they can get better healthcare.
I’ve noticed a resistance in the U.S. and UK to look outside. Both countries appear to believe they are unique or special and are simply unwilling to look at how the rest of the world is doing things.
Almost all the questions and unknowns posed in this article can be answered by simply looking at neighboring European countries and seeing if they’re seeing the same levels of non COVID excess deaths.
I’ve really been amazed at the lack of curiosity and ability/willingness to hold multiple probability-weighted points of view at once and examine questions like “what would have to be true/false in order for us to commit to X?”, “once we’ve started to do Y, what would be the signals for us to stop doing Y?”
I had thought that people were often impatient and disinterested in hard thinking, but the extent of it surprised me, from people of all backgrounds and abilities.
I think one issue, at least from an online experience, is that a multi weighted view just means that you get yelled at by everyone as people seem to look for points of view they don’t like and engage with them from that angle. They will often entirely miss what you agree on, or worse assume any common ground was some ruse to slowly introduce more extreme points of view.
It seems to me that most people are able to think in terms of probabilities (or degrees, more generally) most of the time. Those people need to split the world into safe/dangerous, good/bad, likely/impossible. Also, they tend to not gradually update beliefs based on data the way Bayes' Theorem would dictate, but will often go directly from one extreme to the other.
Some will tend to add an additional level of "unknown", but even in that case, they tend to go for "as likely as not" 50/50 odds, not 80/20, 90/10 or 99.9/0.1, based on evidence.
Maybe doubt/uncertainty is too much of a cognitive and emotional load?
For topics that are also seen as essential symbols of some social group (religion, culture war side, nation), the number who will admit shades of gray fall even further, of course.
According to Eurostat Portugal "recorded an excess mortality rate of 23.9 %" in June 2022. "Other countries with rates over 15 % were Spain (16.7 %) and Estonia (16.2 %)." Overall: "Following a peak of 26.5 % in November 2021, in June 2022 excess mortality in the EU decreased slightly compared to the previous month, to 6.2 %." Bulgaria, Czechia, Italy, Hungary, and Slovakia recorded little or no excess deaths.
Romania (from where I’m from) recorded the least number of monthly deaths in June 2022 since at least 4 or 5 years (I’m on my phone, I have the Excel file with the stats themselves on my computer at home), and, comparing June 2022 to the average of June months for the 5 years before the pandemic, we had 15% less deaths (so you could say we had 15% “less” excess deaths, if that’s even a term).
The explanation is simple, most of our excess deaths happened during the pandemic itself, October 2021 had close to 100% more excess deaths compared to previous pre-pandemic October months, and while that was the worst month for us in terms of extra deaths there were still others with 30-40-50% excess deaths.
In other words it looks like, to put it bluntly, many of the people who would have died in June 2022 out of non-Covid causes had the pandemic not existed actually died in 2020 or 2021 because of said pandemic. In countries like Spain or Portugal not that many people died during the pandemic, hence those countries are now getting “out of it” with a weakened populace, a populace who dies “more” because of that “weakness” generated by the societal effects of the pandemic (less access to face-to-face doctor consultations, for example).
A true science-based society will try to look at all these numbers in 5 years’ time with a neutral mind, so that when the next pandemic comes we will be better prepared to make decisions about lockdowns (“is it really worth it to close everything down if people will die nevertheless when the pandemic ends?”), but I have a feeling that won’t happen.
The increase in excess deaths follows an uncharacteristic decrease from the start of the pandemic. I'm not sure how much of it is a real increase rather than the inevitable being postponed by enforcing very strict disease-preventing measures (social distancing, washing hands, shutting down busy places, etc.).
The weekly numbers for the excess in mortality very much suggests that the death rates for 0-14 year olds were significantly lower in the last quarter of 2020, and significantly higher starting in the middle of 2021, when COVID measures were (starting to be) lifted in large parts of Europe.
I hope the cause behind the rise in death toll amongst children isn't the same as that during the Spanish Flu, mainly that the virus mutated to be mild for adults but deadly for children.
Yeah that's not really a topic you want to look into unless you've a stiff drink to hand imo, a painful amount of I told you so style learning to made picking that apart...
I don’t find that strange at all: vaccination/deaths of the elderly meant the virus needed t9 find a new susceptible population. Spanish Flu did the same: started out hurting adults, ended up killing kids.
We have the same issues in Canada with our public health system. No one wants to talk about this, but my unpopular opinion is the real problem is our retirement program and lack of fertility - we're way too generous, and without a tax base there's only so much we can do.
Unless a politician actually makes the unpopular move to cut retirement benefits or massively increase fertility this is only going to get worse.
Solving the unaffordability of housing crisis is the step needed to unblock fertility.
The solution exist, yet it cannot be pushed forward in a democratic system as it creates a generational conflict.
Although I agree solving the housing problem will help fertility (personally I'm waiting to have kids until I get more permanent housing) it's definitely not the only thing stopping people from having kids. Rich people famously have low fertility and they don't have any trouble getting housing.
Fertility, like homelessness, is a multivariable function that requires a multitude of policies and approaches. It's not a simple dial that one can move back and fourth.
> If the current trajectory continues, the number of non-Covid excess deaths will soon outstrip deaths from the virus this year – and be even more deadly than the omicron wave.
I have friends in the UK and the USA who all during the pandemic were asking, what about the unintended consequences? Where are the models for the impact of these decisions? What are the numbers of collateral damage?
There were no answers. Anywhere. That simply doesn't make rational sense.
What unintended consequences are we talking about here? The problems in the article don't stem from lockdowns, they stem from delays caused by capacity problems in the healthcare system.
So, if anything, the article describes the unintended consequences of those who deliberately kept fighting all measures to curb the spread of COVID.
I can't speak for the nation as a whole, but during the third lockdown, my mental health went through the floor. I stopped exercising, became agoraphobic and developed panic disorder.
It's about a year later now and after a ton of therapy and medication, I'm just about able to go outside again. I still can't really travel far but I managed to drive 2 miles yesterday and am really happy about that - though I did vomit afterwards. Unsurprisingly, my physical health is a lot worse now. I feel like I've aged a decade.
It seems pretty obvious that there are multiple contributing factors, including both long-standing capacity issues, the long-standing obesity issue, and the unintended consequences of lockdowns.
Don't worry, in 5 years we will likely read how those in charge then spoke out but we're silenced and how they knew all along and fought the good fight for us in their ivory towers...
It was a simple mathematic close airports not schools of you're so concerned but the past is now behind us.
Oh and did you know the GBD was secretly funded by evil big right wing oil against the family friendly big pharma with asbestos in the talc and roundup in your food...
(Sorry I think I got a bit cynical even for this topic)
So, if they don't die in the first wave of COVID, they need to die of underfunding?
I mean sterilizing immunity through infection is now known (through many thousands of documented re-infections and likely hundreds of millions) to be both irresponsible and a failure. However, if the goal was to reduce the long term cost of the British medical system through the death of it's oldest and most expensive, then perhaps there is still hope by simply reducing funds?
> I mean sterilizing immunity through infection is now known (through many thousands of documented re-infections and likely hundreds of millions) to be both irresponsible and a failure.
Infection is documented at being more effective at protecting you from reinfection and from having serious complications from a subsequent infection. Let's not pretend that the Great Barrington Declaration was necessarily wrong, given the suffering supply chain disruptions are now causing, not to mention the excess deaths from untreated conditions and increases in substance abuse. Only hindsight will give us a proper understanding of which choices were better.
Note that while this article is listed as being from Yahoo it's actually sourced from The Telegraph, a right-leaning paper that appears to be on a bit of a crusade at the moment to "right the wrongs of lockdowns" or something.
That's not to say there isn't a story here, or even that they are wrong; just be aware there appears to be an agenda.
It's fantastic that it's now even acceptable to talk about the downsides of our collective responses to Covid, something we can thank those trailblazers for.
I'd say pretty similar overall, though the UK had a massive peak and then a sudden deficit in excess mortality where other countries didn't. France and Ireland haven't reported an uptick in excess mortality but their data hasn't been included from right around the most recent sudden rise.
The pattern seems to be that there's an increase in excess mortality, with peaks following drops a few months later coinciding with COVID spread. Sadly, this website doesn't show any data prior to January of 2020, but excess mortality rates were down right up to the spread of COVID.
The US preliminary numbers suggest that since the end of the Omicron wave excess deaths have hovered between 0-5% (compared to 30% or more during major waves). A couple percent is likely still Covid suggesting that the underlying trend hasn’t changed much.
Are there still major pandemic restrictions in Britain? Lots of quotes in this piece seem to imply there’s ongoing issues here but everything I see in Europe or the US from abroad seems to heavily imply that people are “back to normal” (at least in terms of movement).
The idea here (treatment delays lead to excess deaths) seems ok, but is it really the restrictions? Isn’t it more that hospitals are still extremely full? Or is that no longer the case.
The main claim of this article feel a bit… odd to me. There’s a heavy implication about this being from the lockdowns, but in the middle there are 3 lines with a much simpler explanation: Covid infections increase risk of other health issues.
> Are there still major pandemic restrictions in Britain?
No.
My impression is that in the UK (just as in other countries to a degree) the healthcare system hasn't really gotten out of the overload-state ever since the COVID waves. So while delays due to lockdowns certainly happened, it's also an ongoing crisis independent from that. (and if I'm being cynical, advocating for fixing those issues doesn't fit various pundits' agendas because that would mean spending more resources on the healthcare system, so it gets ignored - certainly the silence about this here in Germany has been interesting)
The medical industry still hasn't got out of the covid mindset.
Doctors are still working from home. Hospitals are still refusing visitors and requiring a week of self isolation before a patient comes in. Staff are still isolating for two weeks if they test positive. They still haven't put back full seating in waiting rooms and refuse to let you in the hospital if you're 10 minutes early for your appointment.
Frankly, dealing with the medical establishment right now is a pain - and I suspect people are avoiding it.
I know people will say covid is still around, which is true, but we are ~all vaccinated. This is as good as it's going to get.
Either it's time for hospitals to return to normal and stop using covid as an excuse, or we have to admit as a society that our risk tolerance for infectious disease has dropped considerably, stop treating this as temporary and reorganise things to be efficient again.
Dropped considerably? I'd say our risk tolerance has gone up, not down.
On top of that, the underlying risk has gone up. This is not a good combination for our healthcare systems. They can't get out of the COVID-19 mindset, because they're still dealing with COVID-19.
> I know people will say covid is still around, which is true, but we are ~all vaccinated. This is as good as it's going to get.
We can do much better than this. Something like 80% of the population has been vaccinated, which is far lower than it could be, and we aren't giving regular booster doses like we do with the flu. Almost nobody is wearing masks in public spaces. We should be improving ventilation in all public buildings, but we aren't.
Things could be a lot better -- but our tolerance for risk has gone up, so we're not doing any of this.
Covid is low risk now, due to less lethal variants and immunity. It still kills people, typically unvaccinated, elderly and unwell. However, so does seasonal flu and bacterial pneumonia and yet, prior to covid, the hospital never required a negative flu or bacterial pneumonia test, generally didn't wear masks, allowed visitors and would see you in person rather than just a phone appointment.
It still remains to be seen how many people Covid will kill annually over the long term, but currently most of the people dying from Covid are the same people who would usually die of flu or other usually minor illnesses. Flu deaths have been significantly lower than typical, and until recently, we had negative excess deaths. It's now positive again, but as the article says, the current view is that's due to the medical backlog and not deaths from covid.
> because they're still dealing with COVID-19.
They're not really. My partner is an ICU nurse, and the nurses and doctors themselves largely don't think about it much now unless they're treating it, which isn't that common. Covid used to be something they'd be talking to me about every day, now I'm not sure they've mentioned it in the last month. Doctors and nurses are having work parties with none of them wearing masks. Only about 10 patients a day are admitted to the ICU due to covid across the whole country, and most of them are for reasons other than covid. Again, those are usually the patients who would be very ill from flu. Think 85 year olds with comorbidities.
They are still dealing with it in the sense that any time a patient tests positive for covid, they still send a bunch of the staff who had contact with them away for two weeks. Sometimes some of them end up very slightly ill with covid, and a few others test positive without symptoms. Which, again, nobody ever did for flu, despite it killing more than ten thousand people a year. Many of the staff think this is silly, but given the pressure they're working under due to staff shortages, few complain about two weeks off.
> We can do much better than this. Something like 80% of the population has been vaccinated, which is far lower than it could be,
Rising up to about 95% in vulnerable populations. It could always be theoretically better, but if the remaining people are unwilling to take the vaccine, then that's where it's going to stay. The covid vaccine uptake is approximately the same as the seasonal flu vaccine uptake overall, and by demographic, is higher. Overall uptake has wildly exceeded expectations.
If you just look at antibodies instead, 96% of people have detectable antibodies and 70% (likely more) have actually had covid already.
> we aren't giving regular booster doses like we do with the flu.
We don't give everyone the annual flu booster. Most healthy people of working age don't get the flu booster each year. So far, everyone has been offered the vaccination and one or two boosters.
We also currently have a new autumn booster programme being prepared for the Omicron variant.
That means that by the end of this year, Covid will have been around for three years, and vulnerable people who would be eligible for the annual flu vaccine would have been offered five Covid vaccinations.
Between how widespread it is, how easily it transmits and how likely it is to seriously mess you up, it's not really low risk. Even if it was low risk, it would still mean that the underlying risk of infectious diseases in our society has gone up. Returning to our previous practices would require our risk tolerance to have gone up, not down.
> [We don't do that with the flu.]
I do think we've historically been too blasé about the flu. We ought to be treating it more seriously than we do -- a lot of those things you say we don't do with the flu are things we perhaps should be doing.
> We also currently have a new autumn booster programme being prepared for the Omicron variant.
It's only available for above-50s. We can do better than this.
There are no longer any pandemic restrictions in Britain. But there is still a huge backlog for health treatment, which was largely caused by access to non-urgent healthcare being partially shutdown over the pandemic.
Our healthcare system was in a very big mess before the pandemic. Now it’s in even more of a mess. So it was a case of restrictions tipping it over the edge.
> much simpler explanation: Covid infections increase risk of other health issues.
Or even a simpler one: The discouragement from doing sports that was lockdowns and curfews, encouraged asthma, obesity, breathing interior paints too much, couch potating, mental breakdowns, social isolation, lack of parties, lack of pleasure in life, looping on negative thoughts, eating butter and sugars by buttloads, and not being able to see doctors when needed. Also, loss of work, stress of uncertainty, requirement to change careers for hospitality people.
It’s incredible how much we neglected humans during this whole “let’s protect humans from THAT ONE DISEASE” psychotic episode.
I do not believe your explanation is simpler. At least not without more evidence.
The main reason is that all of the lockdown and curfew stuff was 2 years back now! Most people have just signed out of the covid discussion and are not doing any mitigation. The "psychotic episode" (your words) ended in like... mid-2021. Why is it all falling apart now?
We are mid-2022. Hospitals are still a mess worldwide, because _they are all still getting a sickness that knocks people on their feet for a couple of days to a week_. People whose bodies get hit by this end up being weaker and more susceptible to other issues. Seems pretty simple!
That is not simple at all, and really far-fetched. Lockdown and inactivity won’t turn a fit human being into a diabetic obese and kill them in 2 years.
There are much more compelling explanations (again, mis-funding, burn-out, decay due to malice or incompetence, amongst others). The problems were plain to see before COVID. The pandemic just pushed the system closer to the edge.
All restrictions ended in April I think. And prior to that the last “lockdown” was first half of 2021 when we were hit with Delta mid-vaccination campaign.
I think we can probably mostly agree this is the national government's fault one way or another. But for me it is complete irrationality to assume we just need to give more money to them and have the government fix it.
The government has been siphoning money from the UK population at an ever greater rate while redistributing it to very large private organisations. It won't change by voting in some other bunch of cronies, they're all in the pockets of a great unelected one way or another.
We need to wake up to the fact we all live in a facist oligarchy which is impossible to avoid when we let governments get this large.
Then why is the UK in particular doing so badly with this? A more-likely scenario is that this is the outcome of prioritising Covid (and avoiding Covid) over all other healthcare since March 2020, which has been a relatively unique factor with how our NHS has handled the pandemic.
Wouldn’t a reasonable hypothesis try to rule out the vaccine? I’m not anti vaccine, I received the vaccine. But if excess death is creeping and it’s not Covid, would t that be one of the first things to rule out? They don’t even indicate that was ruled out, just completely ignored.
Here's my thoughts as someone who's trying to get a paper published that shows that _potentially_ the vaccine is implicated in injuries and we'd like to do more research.
We can't say that! It's getting thrown back at us. We're not saying that it's causal, we're not even trying to propose mechanisms. All we're saying is that using government reported data, we see a signal that suggests that certain adverse events are time and location correlated with vaccine roll outs. Could there be other explanations, sure!
Our successful tack has been to take all mention of the vaccine out of it and just report our organized data (organizing government data is always fun) and just publish a paper of data without even suggesting hypotheses to follow up on (doesn't feel like real science to us).
Once that paper gets in the literature, then we can write a second paper referencing that, and go on from there. It's all a political game...that's delaying good science that can save people's lives!
So my guess with this paper is that they have data, they've thought of the vaccine as an issue. But they have to go with a more politically correct reason to get the data out in the open and then they can follow up later once their data is in the literature.
Edit: why the down votes! I'm not saying that it IS the vaccine, I'm saying that it might be and we should study it. But this does show that once you bring up that idea, the censors come out of the woodwork. So frustrating! When politics stop the questions you can ask, we have serious problems.
Thanks for trying to do good science. It's a shame that asking questions (the basis of our job) has become forbidden on some topics.
> So my guess with this paper is that they have data, they've thought of the vaccine as an issue. But they have to go with a more politically correct reason to get the data out in the open and then they can follow up later once their data is in the literature.
> [article] So what is going on? Experts believe decisions taken by the Government in the earliest stages of the pandemic may now be coming back to bite.
If one reads between the lines, what is the largest "decision taken by the government" that could impact directly health? Vaccines. Of course, since media, big corporations and governments have close ties the truth will take time to get out, if it ever do.
I understand your issue but to say your research saves lives is an overstatement. Your implying that the lack of vaccination will save more lives than Covid infection. The fact that you aren’t trying to propose mechanisms is exactly the issue. You’re stoking more public fear by your “simple observation”. So either provide an alternative, or your potential implication is not important enough to merit a publication at this stage.
> You’re stoking more public fear by your “simple observation”. So either provide an alternative, or your potential implication is not important enough to merit a publication at this stage.
Irresponsible science journalism is stoking public fear, not actual researchers trying to do important work. Stop blocking the important work and go chastise the people really causing the problems.
On our first draft, we tried to tease out some of your concerns about relative risk of the vaccine to covid itself, and even had some _potential_ mechanisms to study. But peer review didn't like that. So we've been cutting and rearranging the paper and finally have a draft that looks like it will go through.
We're not trying to stoke fear, we're trying to see what's really happening.
> We're not trying to stoke fear, we're trying to see what's really happening.
Thanks for your hard work. Politics have entirely abducted reason on this topic. We all so clearly fear that the same certain thing may be true, so we are left doing nothing that matters.
It’s not a “simple” explanation if you take some time to understand how vaccine works. Just because there’s a side effect form vaccine doesn’t mean that the vaccine isn’t the best option.
Your thought process is classic example of zero risk bias.
> why did vaccine companies need absolving of any liability by govts?
We know some people will be harmed by vaccination. Despite that, we need to vaccinate as many people as possible. Because of that, we make it easy for people who've been harmed to claim compensation from a government and industry backed fund, rather than force those harmed people to go through the courts against multi-billion dollar companies with very expensive lawyers.
London exagerates this. I work on 6 figures and can't afford any savings. I've moved into a boat to pay less rent, can you believe! I don't know how the rest of the population does it on a fourth of my salary.
> "Prof Robert Dingwall, of Nottingham Trent University, a former government adviser during the pandemic, said...“We are beginning to see the deaths that result from delay and deferment of treatment for other conditions, like cancer and heart disease, and from those associated with poverty and deprivation."
Behind the statistics, here's one person's tragic story:
"A woman with fast-growing stage-four breast cancer says the NHS has let her down, with delays at every stage of her treatment."
'I've been let down - I shouldn't have stage-4 cancer'
Definitely a drop in EU nursing and health-related staff (up to 87% in post-referendum). This may have been balanced with an increase of non-EU staff, but the direction is still wrong (understaffing increasing year on year).
Here in Germany the health care system is severely stressed particular nurses are hard to come by. Nurses and young doctors were often coming from other EU countries but Covid slowed this migration. I could imagine the situation in Britain much worse due to Brexit and quite possibly and even higher reliance on foreign skilled health care labour.
Domestic people were not discriminated against from training.
Birthrates went down, so supply of labor decreases, so prices have to increase to attract more people to do the desired type of labor. Or if the country is desirable enough, the country can open up immigration to increase supply of labor and keep prices lower than if they had kept immigration closed.
Domestic labor can keep moving onto more desirable jobs while immigrants keep doing the less desirable work in exchange for being able to immigrate. Works well, until birthrates drop too low and/or immigrants stop coming for whatever reason.
Oh, for heaven's sake. It's not that patients delayed treatment. It's not the sodding vaccine. It's emergency medicine collapsing because A&E departments can't discharge. They can't discharge because there aren't enough social care workers. There aren't enough social care workers because a) Brexit, b) vaccine hesitancy, c) shit pay, and d) chronic underfunding of public services in general.
Given that this is an article from the Telegraph, exactly how honest do you think they're likely to be about any of those factors?
You are correct! I was responding to the comedic parent.
However, both the Sinovac and Sinopharm vaccines are very equivalent inactivated virus vaccines with comparable (low) effectiveness against any of the proliferating post Delta vaccines, and vaccination rates in the elderly are quite low.
Which makes my point that there really isn't a good controlled environment where all of this data is easily collected. Even the developing world has received significant vaccination at this point, while politics have made gathering and interpreting the causes of excess deaths challenging EVERYWHERE. Sweden? UK? US? France? Singapore? German? Russia? China? India? Africa?
Some insights from the Netherlands, the country right to the east of the UK: the healthcare system is still under extreme pressure and everyone important is pretending the pandemic is over.
Nurses and other healthcare professionals have been quitting and are not planning to come back because there is no chance of increased pay (which only drives up the pressure to those still working in healthcare).
Hospitals are working through their backlogs. Care that could be postponed has been postponed for two years and now with fewer healthcare professionals and medical issues left untreated for a while (even people starting on chemo got told to wait at some point) the recovery process is slow. This, of course, isn't great for the relatively large elderly population as they're very reliant on lots of healthcare.
I don't know what the state of the NHS is these days, but I've heard distressing signals from all over the UK about people being unable to get a GP appointment in time and the entire hospital system being overworked. I don't know if it's politicians trying to cut more healthcare costs, the pandemic, Brexit, or everything at once, but the NHS doesn't seem to be doing well.
Over here, we have all but stopped testing for COVID. It's seemingly presumed to be endemic by the government, much like other governments seem to do. In every sector sick leave has also been on the rise, as the government told us to expect; the consensus seems to be that the current variants of COVID aren't that much of a risk and we should just go back to normal and let the disease run its course. With reports of long COVID symptoms on the rise [0] I very much doubt that, but the government doesn't seem to care about sick people, so I'm not surprised.
Excess mortality in the Netherlands has been high ever since the start of the pandemic [1]. Every time the virus spreads, excess mortality rises. The covid death rate [2] is claimed to be extremely low but at the same time COVID testing has also pretty much stopped, whereas previously anyone dying with COVID was also written up to have died with COVID. Based on the mortality graphs I'd say we've passed another COVID peak but nobody (I know, at least) takes an official tests so the statistics are very much flawed; wastewater analysis [3] seems to suggest a "hidden" endemic that coincides with the rise in excess mortality, though.
My personal conclusion: we're in (or have just passed) yet another mass COVID spread event but everyone has grown tired of taking any anti-COVID measures, so they stopped caring. I dread to think what the winter is going to look like if the summer death toll is this high. The UK's COVID numbers seem to agree with a similar peak in positive tests but I don't know how well the reporting is done over the pond.
There is also another factor at play: the extreme heat due to climate change we're facing in Europe. In (previously) unusually warm summers or cold winters, old and sick people have always had a tendency to die more often. The heat of the past few weeks definitely isn't the only cause, but I doubt it's not a factor this year with record heat reported all across England.
As an aside: the amount of people here immediately jumping to the conclusion that vaccines are the cause is... quite depressing. We're still very much in a pandemic but everyone just seems to _want_ to blame vaccines while we, as a society, try our best to stuff our fingers into our ears and pretend we can't hear anything. Do whatever you want to feel better, blame the vaccine, blame Bill Gates, blame the lizard people running the Illuminati, but it won't solve the problem.
Many others predicted excess deaths owing to people skipping regular checkups/missing out on cancer treatments, etc etc. This was widely reported and debated as a cost of lockdowns. It's implausible that there would not be excess deaths owing to this effect. In which case, the question shouldn't be: "what is causing these excess deaths?", but "are there _excess_ excess deaths?". I.e. are there deaths which _can't_ be explained by several years of significant numbers of people not seeing their GPs?
Added: I do agree that we shouldn't assume that mRNA vaccines are safe just because we want them to be, and large scale studies are required. But then large scale studies are, of course, happening. There'll be NHS reports on the long term effects of these vaccines for decades.
This bullshit does not resist the most superficial analysis. There were million deaths before vaccines were rolled out and death rates haven’t stopped declining since then. Also, there are plenty of countries to compare to, with similar vaccination rates as the UK.
Different vaccines / drugs / lockdowns / treatments rolled out in different regions. I’m not claiming they’re exactly causing anything, but there are / is a correlation; based on multiple public records
However myocarditis often indicates heart damage. Which is often long lasting, also the CDC just removed the claims the vaccine only lasts a few days. We don’t know how long that spike protein lasts.
Because if the possibility turned out to be true, it would be extremely damaging at a social and political level. Not just on institutions, but on the psyche of people in general. I think everyone understands this at least on a subconscious level. There must not be any truth to it, because if there was, it would do too much damage.
So why would I want people to discuss something that could potentially have that kind of impact? Because I want people to face all of the possible consequences for their choices, not just pick and choose which ones they will consider and acknowledge.
This is teetering on the edge of conspiracy theory. People are and have been researching this possibility and so far haven't found anything big worth reporting. Just because there is no big news doesn't mean people are hiding it.
Remember when simply considering certain possibilities was condemned as proposing conspiracy theories?
"The Lancet letter (also referred to as Calisher et al. 2020) was a statement made in support of scientists and medical professionals in China fighting the outbreak of COVID-19, and condemning theories suggesting that the virus does not have a natural origin, which it referred to as "conspiracy theories".[1][2] The letter was published in The Lancet on February 19, 2020, and signed by 27 prominent scientists, gaining a further 20,000 signatures in a Change.org petition.[3][4] The letter generated significant controversy over the alleged conflicts of interest of its authors, and the chilling effect it had on scientists proposing that the COVID-19 lab leak theory be investigated."
In your assumption that they don't want to consider that possibility. You take your own projection as a given and then continue to argue as though it is true.
1) That's not what circular logic is. Circular logic would be if I said "they don't want to consider it because it's harmful and it's harmful because they don't want to consider it."
2) You asked me why I thought people don't want to consider that possibility, so it's pretty dishonest to now say the premise on which my opinion is based has no basis. If you were arguing in good faith, that's what you would have started with, eg: "People aren't avoiding it" not "Why do you think they are avoiding it."
'“We are beginning to see the deaths that result from delay and deferment of treatment for other conditions, like cancer and heart disease, and from those associated with poverty and deprivation.
'“These come through more slowly – if cancer is not treated promptly, patients don't die immediately but do die in greater numbers more quickly than would otherwise be the case.”
'The Government has admitted that the majority of the excess deaths appear to be from circulatory issues and diabetes – long-term, chronic conditions that can be fatal without adequate care.'
These deaths are attributable to specific causes - chronic conditions not receiving proper ongoing care - which have nothing to do with the vaccines. Hell, vaccines /should/ be increasing the amount of ongoing treatment for these conditions, and helping people get back to regular checkups and the associated preventative / early-stage treatment. (noting of course that the current excess deaths are an extremely laggy indicator. the 'vaccines help' hypothesis should then be apparent in a year or two as the excess deaths come back down.)
Yes, the article does a fantastic job of claiming their hypotheses as the only possibilities, while dishonestly ignoring others that would more severely undermine confidence in the state.
I'm honestly surprised they're attributing deaths to lockdowns at all! That's a huge shift in the overton window. If you remember, that was also taboo. But I assume now it's ok to talk about because it can be framed in the louder, "not enough funding for healthcare" context.
It sounds like you really want it to be vaccines even though not much seems to be pointing towards that conclusion, be careful to avoid a bias. The article mentions cancer and cardiovascular chronic diseases.
Of course it's a possibility, and it has received an enormous amount of scrutiny, before and after approval, in many independent countries. The safety of the vaccines is the most obvious thing to be on the lookout for. But just because some people don't like the vaccine doesn't make it more likely to be the cause of excess deaths. Have you considered that fixating on the vaccine could be blinding people to a whole bunch of other potential problems?
To add to this, there has been evidence that the spike proteins created by the mRNA sequences stay around in the body longer than expected. CDC has now implicitly admitted this.
Why would they? It just undermines peoples confidence in the institution, with no gain. That's the lens that these kinds of things are looked at through. Better to just quietly alter the messaging.
Just for an example, acute organ damage doesn’t necessarily present symptoms immediately. I knew a kid who had a viral heart infection in his teens that severely damaged it. He recovered in the sense that he could mostly live normally, but his doctor told him he’d be lucky to live past 50.
People were repeatedly told to seek treatment when they needed it and not to be put off from going to A&E. It was a pretty regular topic on the daily press conferences.
That advice to seek treatment was drowned out by the "Stay Home, Protect the NHS, Save Lives" slogan that was repeated everywhere, along with use of death/infection numbers that were spun out of proportion by the media.
It is no surprise that people decided that the risk of seeking treatment was not worth it.
Yeah my local doctors' surgery had massive posters in its windows during the lockdown that basically said 'go away'. If you braved leaving your house and going to them, you'd be put off again before you got to the doors.
Routine investigations, operations and treatments for entire categories of disease were entirely cancelled in many hospitals. In the big one near me, most of the big equipment like CAT scanners and such were turned off and mothballed for well over a year, some more than two years. No investigation or treatment for many conditions during this time.
So I really don't buy the "seek treatment when needed" line. The public was both cajoled intensively into not using the NHS, and the NHS itself shut down a lot of its basic services. Not just reduced. Shut down entirely. For over two years.
I'm friends with one of the radiation safety officers who was responsible for overseeing the shutdown and then the restarting and recommissioning of the equipment. The NHS shut down! What we are seeing now is the consequence of that. And we were expected to both pay for it, and applaud this weekly.
I hope that if there is one outcome from this pandemic, it's that we never allow such a situation to cripple the whole economy and the health service in such a way again. The cost of closing it all down will be many times greater than the cost of the pandemic itself. It should never have been done, and we need to look long and hard at the pressures and the decision-making that led to this.
One might even conclude the reason it happened is governments seeking power (lockdowns, propaganda and censorship, travel restrictions, etc) rather than genuine public health.
I think the government and the media had a negative feedback loop.
I've noticed the media prefers to saturate news with one topic. For years it was brexit, then that stopped completely and it was Covid, then Ukraine, now energy price rises.
The Conservative government originally were keen on personal responsibility. But once the headlines started of older people in carehomes dying, there was no hope of doing nothing any more.
Lockdowns were the "something that has to be done".
{kind=link}
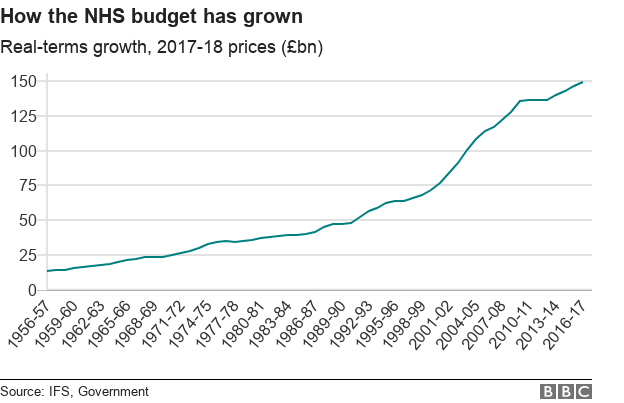{kind=link}
- Getting a GP to see you in person is now quite difficult (they want to do everything via phone). - Seeing your GP (depending on your area) can involve a 2-3 week wait and waiting in an hours long phone queue. - When you are referred to hospital for tests you can be waiting 6-12 months for the most simple things if they’re not life threatening (even if they are life limiting in the meantime).
I personally have gotten to the point where I would not want to live in this country without access to private healthcare. I’ve had a number of treatments privately and they’ve saved me months of pain, anxiety, and in one case outright refusal for treatment by the NHS until the issue became dangerous (which was inevitable).
In the UK we treat the NHS like a sacred cow. Even people who have experienced appalling treatment feel the need to exonerate the NHS when complaining about their experience. While the people that work there are not the problem (the failures of the government are) we need to start calling a spade a spade. The current condition of the NHS is atrocious. It’s not “great/the best health system in the world” and we’re no longer “so lucky to live here with the NHS”. It’s shit and it needs massive changes. Unfortunately without a change in government we’re not going to get those and people are seemingly more concerned about refugees arriving by dinghy than health care.