This article is really informative, and makes me feel proud to be an Indian. Medical care really is one of those things that no person should have to beg or borrow for, in a civil society. We're still not there yet as a country, but the signs are positive.
FWIW, I'm relatively well off and have medical insurance, but the cost is absolutely negligible compared to what I hear is prevalent in the US - about $10 / month.
It's probably just my bad luck, but I've had three surgeries in the last 10 years - an appendectomy, an ACL replacement, and a septoplasty. Each one of these was done in highly regarded (and expensive) hospitals in Delhi - Apollo, Max, and Fortis. Each time I walked out of the hospital without paying a single dime. I just had to show my insurance card, and the entire stay was cashless. In fact, after my last surgery I realised that I could have even been reimbursed for my medication post surgery if I'd kept the receipts (which I unfortunately didn't).
I lived in India for about 5 years and worked in the healthcare space with all the hospitals you mention. So here's my take:-
India has amazing "private" hospitals if you compare the doctors and the equipment they use.
India also has the worst "private" hospitals if you compare the hospital support staff specially nurses. Most of them (not all) nurses have no passion and the profession itself is not given the kind of importance that it is given in the US.
Also, the public hospitals in India are a joke. They are terrible. Although some of the best doctors in India come from there. I guess, after seeing more patients than you can handle and having a free hand to do pretty much whatever the heck you want with zero liability (unfortunately and sadly at the cost of the poorest of the poor) they become good.
In most cities in India the private hospitals have turned into a profit making operation with zero oversight and in most cases governments supporting them in manufacturing patients. I would get a second and third opinion on any expensive procedure that would a doctor would recommend in India.
I made lot of friends who are doctors in India and all of them tell me they get direct cash kickbacks from hospitals and labs for referring patients. This is be highly illegal in the US.
Cleanliness is another major issue in Indian hospitals. Even in the best ones most staff don't follow basic sterilization procedures that are common in the western world.
So all in all its great that the hospitals in India are affordable to a cross section of Indians but they can be better with better government oversight and having well trained and passionate nursing staff which might increase costs.
"India also has the worst "private" hospitals if you compare the hospital support staff specially nurses. Most of them (not all) nurses have no passion and the profession itself is not given the kind of importance that it is given in the US."
This is because Nurses don't get paid well, avg pay will be around Rs 15,000/month which is simply not enough in metro cities.
Majority of the profits of private hospitals goes towards Doctors and hospital administration.
Nurses pay have been stagnant for so long. Nurses don't even get extra pay or shift allowance for working nights. Many of the skilled ones, migrate to western countries rather than stay and work in India.
Nurses do get paid well in govt hospitals, but govt hospitals are so few as compared to privately run hospitals.
I always think that even nurses that are relatively well paid are really underpaid for the job that they do. It is a highly stressful job doing a lot of really unpleasant things under difficult conditions. You have no real leeway for having a bad day -- people suffer if you don't perform. It requires a lot of study, experience and skill to do well. While computer programming is a scarce skill, in no way does it compare with the job of a nurse... and still there is no comparison in salary. And that's for nurses that are relatively well paid. The world really is unfair.
I try to impress on the hospital management during my interactions with them that nurses in some ways are the most important staff in a hospital. They interact with the patient the most and they have the most knowledge of the situation than even the doctor in some situations. Hospitals in the west seem to get this but in India they don't. Most of the focus is on the doctors and equipment. Hopefully this should change in the future.
Even some "public" hospitals are really good. e.g. Tata hospital in Mumbai, They have had equipments and cancer treatments, which are even considered state of art in US. Like DOTATATE scan and lutetium therapy has been available to so many people in India for more than 5+ years now. Only 2 hospitals in Mumbai have it Jaslok and TATA. And TATA charges are so low , its a blessing for all the people who have been able to get treatment. Experience both healthcare system. India is cheaper which means every one can get access to cheap medicines and medical treatment. US obviously will fare better.
For those like me who were confused : The Tata hospital was originally commissioned by a philanthropic trust established by one of the Tata's, arguably one of India's most famous business families, and also possibly the most active in philanthropy / social welfare. The Tatas are also responsible for some of India's best research institutes - TIFR / IISc, as well as places like TISS, NCPA.
> Also, the public hospitals in India are a joke. They are terrible. Although some of the best doctors in India come from there.
How can they be terrible and have the best doctors at the same time ?
> Cleanliness is another major issue in Indian hospitals. Even in the best ones most staff don't follow basic sterilization procedures that are common in the western world.
You mentioned before that some private hospitals are amazing, yet here you mention that cleanliness is an issue in indian hospitals. How can they be amazing if cleanliness is an issue ?
> So all in all its great that the hospitals in India are affordable to a cross section of Indians but they can be better with better government oversight and having well trained and passionate nursing staff which might increase costs.
Are you saying that all the nurses in the US come all 'passionate' ?
>How can they be terrible and have the best doctors at the same time ?
If I'm understanding correctly, public doctors are in a good position to get experience in dificult cases and learn from worst cases before to jump to private hospitals
I have a problem with the idea of "passionate nurses".
Nurses shouldn't be "passionate", they have to be professional. Passionate people, unable to emotionally detach, will burn quickly in such place like an hospital (where the supply of suffering people is endless, and they can't decide and bassically obey orders from the upper staff). This has lead in the past to compassionate serial killers. Death angels have always the best intentions drawn in their head. Trying to be the mother and best friend of each one of your patients is a terrible strategy at long term.
Without ever having been to a hospital in India, presumably the doctors go in not-very-good, then when they become excellent they move to a private hospital.
When I look at what surgeons actually do, it seems clear to me that more than anything else they need lots of practice. Life isn't very fair, so I'm guessing most of the practice happens to poor patients and most of the competence happens to rich patients.
I am not saying you should not be proud of Indian progress, but I suspect the experiences of a businessman in a big city in India are vastly different to a low caste woman with TB in rural India.
A friend of mine is a nurse who did social work in rural India. What she told me about the local hospitals was horrifying, not just the condition of the hospital and how patients with infectious diseases were sleeping on the corridors because of lack of beds, but how the doctors had a total disinterest (bordering on contempt) of the uneducated woman who she went to appointments with.
Experiences in India will vary dramatically based on which state you live in. If you are rural Kerla, a state with 50M people in South India, you are likely to get some of the best quality healthcare are very affordable rates.
It’s hard to generalise anything about India which is incredibly huge and diverse.
Kerala is but one state out of many. Kerala is probably the only state in India with a public safety net. How many states names can you pull to exemplify your argument besides Kerala?
Reminds me of Amartya Sen's quote "...whatever you can rightly say about India, the opposite is also true".
A lot of systemic issues will only be resolved as the society progresses, and there is a long way ahead for India.
The use of the word "low caste" is in quite mean considering "poor" would be more appropriate.
Just as Black or Native American would be a poor substitute for poor american.
Or Roma/Eskimo/Greenlander/Sami for Europe
Especially considering that the current prime minister and president of India are from so called backward communities.
India has come a long way in social development and using the "caste card" is quite out of taste.
The word "Caste" is of European origin and does not have a proper native equivalent.
The "caste system" itself is again a European concept imported into India to aid the colonial powers in their divide and rule.
Unlike the persecution of the Native Americans, Blacks, Jews or Aboriginal which were systematic state run pogroms often in democracies.
The fate of the "low caste" can be attributed to the fact that they were the most exploited, often to the point of death or slavery under colonial rule.
While the so called "Upper caste" enjoyed second rung positions as peons, clerks and teachers. This experience is universal in the other colonies like Rwanda, Syria or Iraq where the words "Tribes" or "Clans" have come to substitute "Caste".
It must be noted that the newly independent India gave all Indians of both sexes the right to vote and went on further to provide "reservations" the equivalent of "affirmative action". This was long before the black American even got the right to vote. Less said about Europe the better, the "Roma" still get rounded up and "deported" even though as EU citizens they have the right to mobility.
"Caste" is a powerful tool for the unscrupulous politician inside India. The excuse of colonial apologists or more markedly the evangelists (if they are not the former) outside India.
Caste a European concept so prominent in the family names of Americans and Europeans, has today become synonymous with India thanks to the relentless propaganda of the colonialists/evangelists.
It is not out of taste. Caste System(Jati System) though weakened still alive and kicking in India. (Dalits) Lowest caste layer in India is still subjugated to things like Cow vigilantism, Honour killing, Social boycott, Caste clashes and discrimination in various/all forms of life. It is interesting to note that Dalits are almost always on the receiving end of these issues.
Giving example of the Prime Minister/President is equivalent to saying since Barack Obama is the president of US, black discrimination.
PS: I belong to the so called Lower Caste in India and I have myself experienced instances of subtle/blatant discrimination. Thankfully haven't experienced anything serious yet, maybe because I became an Software Engineer and now live in a major city, thanks to the affirmative actions adopted by India, but poorer strata of lower caste living in tier-3 cities/villages face a lot of cases of discrimination even today.
While India has a long way in social development, it still has a long to go. This narrative of bashing Europeans/Outsiders/Pakistanis for anything negative has to stop. Jati System has been in practise for thousands of years now.
> I became an Software Engineer and now live in a major city, thanks to the affirmative actions adopted by India...
You mean from reservations in school / university admissions? Or does that even extend to private employment? Is there widespread resentment?
I'm really curious about the parallels (or not) between racism in the US and caste in India, esp. affirmative action. The US never really went all-in on AA like India did with reservations -- more like pretending if we mostly ignore race then racism will go away -- but it seems like neither approach has really gotten to good place (yet).
If you’re interested there’s an interview on the Brown Pundits Podcast, “The Life and Views of a Middle Class Indian Dalit”,
> In this episode, I had a conversation with a middle-class Dalit who lives in Gujarat. For me, Dalits are people who are reported on, written on, people who I hear about spoken of (usually sympathetically). But I wanted to talk to a Dalit who was a university educated middle-class person, to zero in on the essential aspect of being SC in India today. At least urban India.
> One interesting observation is that his own experience in India is filled with slights, but not day to day oppression. It doesn’t seem the lot of Dalits in urban India is anything like that of black Americans during Jim Crow. He seemed to assume that America had solved much of its race problem and that that’s what Dalits should aspire to. Curiously, Americans at this point, at least on the Left, perceive our racial problems as dire.
Yes, there are registrations in university admissions, which is the one I used. It does not extend to private employment. Regarding the resentment part, yes, people have resentments against reservations, though now even higher caste groups have started demanding reservation - this means the community will call for strike, stop trains, buses to get the attention of the government. OBC reservations in India were started in 1980 after a similar country wide strikes.
Ignorant question: in India, how can a stranger know your caste? These days I assume there is some mobility, so is it possible to say move to Mumbai, dress the part, and rebrand yourself as a higher caste?
I’m in US, race is the thing here and it’s fairly identifiable.
In many cases your surname/family name can give away your caste. There have been social movements in the country where groups have shunned the practice of using their family names that are used to identify caste.
Well there are many ways, most of the Hindu surnames are representatives of their castes- for example Sharma means High Caste Pundit, (Agarwal, Agerwal, Agrawala, Agarwala, Aggarwal, Agrawal)-> all mean a Bania(Trader) Caste etc etc.
Apart from that, you are required to submit your caste certificate in school in for Board Registration, which is loosely handled, hence process is not anonymous, so now your schoolmates know your caste.
In my College, there were many ways to know the caste of the person- like Fee structure is different for SC/STs and Others.
The whole list used to be published publicly, and everyone had to refer to it during semester registration. Now everyone who notices your name knows you an SC/ST.
There was huge resentment in the General/OBC community regarding the Fee Structure, as they just see that his mate is paying almost 1/10th the fee. I usually didn't reveal my caste to anyone, and my surname is a bit ambiguous so sometime my peers/friends used to rant about it as well.
Now after college, I have lived in around 3 major cities- Mumbai, Delhi and Bangalore. Usually no-one asks about your caste here, but it does happens sometime.
People belonging to Higher caste have no issues in revealing it, though people in my/lower communities usually hesitate and do not want to reveal it.
Moving to other city and rebranding yourself as an higher caste might work, but if caught, there can be social severe repercussion. Caste hierarchy is actually flexible and dependent on the social position of the caste in that specific area. So you would also find cases, where X is a higher than Y in some places.
Arranged Marriages in India are most mostly caste based as well.
People also associate caste with IQs as people of lower caste using reservation didn't had to score much in their entrance exams, hence usually I avoid the topic all together if possible. There are other traits as well that people assume.
Now not everyone would discriminate against you, its almost like not every white guy is racist in US, but you would very much like to just avoid interacting with the ones who are.
But I would still say an inherent Bias is still present.
In short, answer to your question- yes rebranding yourself is possible, though its not very simple. There is even a term for it in sociology named Sanskritisation. There is also Brahminisation, which is when a group adopts social traits of Brahmins who sit at the top of the caste system.
I'm very confused by your comment, and I hope you can clarify. I'm familiar with the colonial/European origin of the "cast system", but having been to India a few times and studied/read a bit, saying that the word has no proper native equivalent (to be blunt) seems both irrelevant and kind of disingenuous. Regardless of the word's origin or colonial reasons, it seems clear that caste-related issues are very visible and very present in India today. Do you agree? You seem to admit as much. But you also seem to downplay the entire existence of caste.
I'm really not familiar with the tribe/clan system in Iraq and Syria. My experience in some other former british and french colonies made it clear how the colonial system benefited from or even created and promoted ethnic rivalries, racism, tribalism -- yes absolutely -- but none of those situations seemed to really be a direct analogue of India's caste system. Do most people in India think of caste pretty much the same way as Americans think of ethnicity or racism?
Maybe you can also talk a bit more about Modi and his "low caste" background, because I've been curious about this myself. How much do you make of his "caste" as part his political identity? Do you see this as a sign that the caste system is dead/irrelevant/never-existed? Or that the low castes have triumphed? Or is he a pawn/token in a bigger game?
If one has Anglo-Saxon family names like Smith, Farmer, Clark or the Germanic equivalent like Meyer, Schumacher etc, it is often the profession handed down father to son. In India this is termed the JATTI, and is considered the nearest equivalent of the caste.
If India was the only country where "caste" is a phenomenon, at least we should have a native name for it. People often claim Varna to be the equivalent, but you almost never hear the word "Varna" being used.
The reason is "William Jones", who synthesized the Indian caste system by selectively digging deep into the scriptures.
Caste today is essentially an economic mobility problem and should have a quick death. But by constantly casting it as a social problem people make sure it is kept alive.
The main beneficiaries are
1. Politicians
2. Evangelists
3. Otherwise wealthy Indians who have managed to carve out a quota from the reservation system meant to benefit the backward communities.
4. Used as a stick by the west
5. Naxal and sociologists
Modi unlike Obama isn't a one show man. Nor is he just the face of the party. He has won again and again, and continues to have huge public support. Goes to prove ones caste isn't important to the public.
Caste is also extremely regional, the names are meaningless outside. In the state that I come from TN, the vast majority of the people have gotten rid of the their family names for the last 2-3 generations for the sake of social equality, yet have a 70% reservation.
Understandably JATTI (rather than caste) is significant among the poor because it is their primary social security. So fishermen, metal workers, farmers, weavers etc form a strong community within their profession.
Like a lab rat that has been deliberately infected and the conditions made worse so it can be studied. The "caste system" that should have a natural death, continues to live on thanks to our heros.
What do you mean caste is a European concept? Hinduism has the four varnas and Dalits. How are those European concepts? Europeans didn’t invent varnas, the avarna, Hindu purity concepts, or the jatis. The jatis are Islam so for Europeans to have invented them would be quite impressive.
My wife is a physician. Four weeks ago she was in severe pain and could hardly walk. She drove herself to the ER at the hospital system that is also her employer. After getting admitted at the ER, the first person she saw was a lady to collect her $150 copay... While in severe pain and before seeing a care provider. That's the current US healthcare system.
She ended up having emergency spine surgery. Fused L5-S1 vertebrae and replaced disk in between.
The US healthcare system is absurdly inefficient but the nominal cost comparison given in the article is meaningless since wages make up a huge proportion of costs in healthcare (either directly or embedded in supplies and services.)
Nominal per capita income in India is ~$2000 while in the US it is ~$60,000. Simplistically one would expect costs to be approximately 30x higher in the US so a 20x difference in cost of $200,000 to $10,00 doesn't seem absurd.
Agree. I have seen estimates place purchasing power parity of USD in India as 0.3, implying that $100 spent in India purchases as much value as $300 in the USA. This would imply a $10,000 surgery in India is somewhere in the realm of $33,000 in the USA.
I have no idea on the DRG associated with pulmonary thrombectomy to even estimate what Medicare allows for reimbursement, but it’s not going to be $200,000. If I find it, I will reply to this comment with an estimate.
I looked into the data. This would probably be under DRG 252, 253, or 254 (DRG 252 OTHER VASCULAR PROCEDURES WITH MAJOR COMPLICATION OR COMORBIDITY, 253 OTHER VASCULAR PROCEDURES WITH COMPLICATION OR COMORBIDITY, 254 OTHER VASCULAR PROCEDURES WITHOUT COMPLICATION OR COMORBIDITY)
Covered charges for 2016 ranged from ~$64,000 to ~$110,000, with ACTUAL average total payments ranging $13,000 to $26,000.
This article is using differences in purchasing power parity AND the difference in charges / actual payments to generate an eye-popping headline. At the actual data level, India is more expensive compared to the US.
Hospitals usually lose money on Medicare and that’s part of the reason other payors have to pay subsidy rates. Not saying they pay sticker price they are billed but I doubt 13-26k is the average reimbursement for any procedure that ties up an OR for a full day (according to the article).
Inpatient care for many major procedures are bundled under Medicare. This is actually the reimbursement for the entire hospitalization.
Yes many places lose money in Medicare as it probably reimburses at around 80% of cost but it’s the only data we have, so it provides the closest thing to a national comparison.
My point is that what this article ultimately shows is that the cross border comparison can generate striking numbers but almost all articles like this never place the Indian “cheap” numbers in context.
Compared to high margin low volume surgeries in the US, this is low margin high volume. Its ingenious how the highest skilled individuals only step in for the trickiest part of the surgery, but the simpler tasks like getting to a heart are performed by lesser doctors or nurses.
Some things make sense like having medical machines maintained in house. Other things, like sterilizing and reusing IV lines seem pretty risky. But perhaps the risk is approachable in this case since a patient is less likely to sue if complications arise from something that could somehow be twisted into a jackpot lawsuit?
Assembly line approaches to surgery are not unique to India. The Russian ophthalmologist Svyatoslav Fyodorov who pioneered the radial keratotomy (correction of myopia by reshaping the cornea) in the 1970's founded an institute - the Fyodorov Eye Microsurgery Complex - that performed radial keratotomies in an assembly line manner [0][1]. Operating tables would literally be rotated from one surgeon to another. At the time, surgical correction of myopia in the West was fairly unknown, as opposed to today where ads for Lasik are blasted everywhere.
Sterilizing and re-using IV lines definitely carries some risk. The alternative to that "risk" in India seems to be letting most not-rich people die because they can not afford to do those things differently. And the Indian health service is telling him he's _still_ costing too much. The result will be taking more risks, with some people paying the price for them. Because that is what India can afford.
Meanwhile, in the U.S. we can afford spending two orders of magnitude more. Something is not right.
> Its ingenious how the highest skilled individuals only step in for the trickiest part of the surgery, but the simpler tasks like getting to a heart are performed by lesser doctors or nurses.
Having observed a few major surgeries in the US, this appears to not be a unique practice and doesn't explain the pricing difference.
The difference here is not that we don't do surgeries efficiently, but that we are subject to the effects of regulatory capture, which stops any kind of price competition in its tracks and leads to $300 bags of saline.
I most am most likely going to need an ACL surgery in a couple of months so we will see how it goes. So far I found out that pretty much every "X is difficult" is a gospel peddled by lazy. This is my first relatively major incident so I'm running pretty blind -- I'm approaching it as I approach needing to do something in business.
Instead of going to the ER ($2,500), I went to a walk in medical center ($120), got seen by an emergency medicine doc. I got a $120 (ER) brace for free in that clinic -- it is probably one of 100 in NYC, open 7 days a week from 8 am to midnight -- i did not go to their other one which is 24x7
Instead of spending $800 on X-ray at the ER, I spent $40 and got results on a CD within 10 minutes at the same walk in clinic.
My MRI was not $2800 but $600 because instead of doing it in a hospital I did it at the radiology center. Both the doc at the walk in clinic and the surgeons said "You can do it in the hospital but it would cost a lot more and take a lot longer. Go to Lenox Hill Radiology -- they have about fifty locations in the city and you would be able to get it done today oh and your results will be emailed to us".
My two visits to orthopedic surgeons ( there were two different doctors working at the same office ) specializing in sports medicine ( fixing athletes ) cost me $260 ( first visit ) and $120 ( follow up ) -- same two surgeons looked at me and the second visit included a second set of X-rays ( not extra cost ).
My one on one PT specializing in sports rehab is costing me $100/h rather than unknown amount.
I have a hunch simply because I let my fingers do the Googling my ACL surgery wont cost me $50k even though I won't be leaving NYC to do it.
What is that magic thing that I did? Googled "Sports medicine surgeons" and sent emails to the email addresses. I also googled "Physical therapy near me" and emailed all of them, getting the prices and asking if they had any experience with rehabbing athletes -- I read reviews of the ones that did not respond after -- none of them had good reviews. The ones that did respond had very decent prices, used tech and were on the ball oh and they had stellar reviews.
But I guess that is hard.
Edit: Cute. Bring on the downvotes. That's the crux of the problem. Personal responsibility is "hard" so no wonder those who tend to outsource it get fleeced. When HN re-enables my posting ability I will respond to the individual questions/positions.
What happens when someone has an emergency like a stroke or heart attack? Not a lot of time to email all the local hospitals. What happens when the patient is unconscious? What happens if their condition can only be treated by a certain facility or medication?
But yes, surely people are only getting screwed over the healthcare system because they are lazy. /s
That's the only time when one cannot get quotes. Depending on a location ( ave/st in NYC and a time of day ) the ambulance would take one to a specific emergency room in a specific hospital chain.
But again, that's not where most of medical services "waste" is occurring.
It's both the duration and increasing severity that account for much of the cost, along with the systematic cost-inflating aspects of the US healthcare system.
That's just hand waving. If the duration increases it makes absolutely no sense not to attempt to get the cheapest way to manage the condition.
People do it all the time if they are on a hook for payments -- that's why we have drugs being grey important from Canada, Europe and India, especially if those drugs are not covered by the US insurance. Suddenly saving $200/mo per type of a pill becomes important. As soon as it is covered by insurance it becomes "Whatever, insurance pays"
Actually, the best cost-containment strategy is to make the provider liable.
That's the notion behind comprehensive HMO systems, with fixed capitated premiums, minimal copayments (a very low friction suffices against most frivolous use0, penalties for failed delivery (see also the Chinese doctor model: the patient pays when healthy), comprehensive monitoring and routinisation, a public health model, and som external oversight.
Within the US, that model describes the Kaiser Permanente healthcare model. Or Medicare I'd add a Danish malpractice remedy to that (provision of care to correct or mitigate mis-delivery or errors), but it's remarkably effective.
Pharmaceuticals remain outside the Kaiser and Medicare systems, a chief weakness.
There's also the fact that virtually all improvements over pre-modern longevity come from public health rather than acute medical interventions.
> What happens when someone has an emergency like a stroke or heart attack? Not a lot of time to email all the local hospitals. What happens when the patient is unconscious? What happens if their condition can only be treated by a certain facility or medication?
This is not a rocket science: when one sees a complex problem one does not attempt to solve the entire problem using an full rewrite -- instead one breaks out it into pieces and solves one piece at a time. If the piece is too big to solve that piece is broken down into pieces and those individual pieces are solved.
It is debugging of the problem 101.
> What happens when someone has an emergency like a stroke or heart attack?
Call 911.
Have a toothache? Don't call 911. Call a dentist. In fact, call several dentists. It is, of course, possible to call 911 and have an ambulance take one to an emergency room because of a toothache ( this was a case told to me by a friend who is currently doing an ER rotation. He swore he was not pulling my leg ).
> What happens if their condition can only be treated by a certain facility or medication?
It is unlikely that a common condition can be treated by a single facility.
> or medication?
If we are to optimize the costs of overspending by not selecting cheaper alternatives where we can there would be more money to spend on the expensive "it can be only done here" or "it can only be done using this medication".
That's very interesting information, but I could have done without your snide allegations of laziness towards everyone not in your fortunate position - being both educated and confident enough to research and negotiate pricing, and having a relatively non-urgent problem. The last time I was in the ER I woke up there with no clue as to how I had arrived.
Most of the problems in the health care are non-urgent.
Most of people at the ER are not there "waking up and not knowing why they are in the ER". They walk into ER with something not working for them. That's exactly why it takes 3-4 hours to be seen by the ER doctor.
People like you, who wake up in the ER, are rarities. Those people are either brought to the ER in ambulances or are triaged and seen immediately. It is for those cases one could justify the costs of an ambulance ride and 500% markup of an bandage.
I do not agree that most visitors to the ER do so for non-urgent reasons, although few complaints are so severe. I don't think you've fully grasped the point people are trying to communicate to you here.
Sibling commenter is correct. The majority of ER visits are actually not emergencies; rather they are frequently used/abused as a convenience (open 24/7) or because payment is not required prior to care due to the unfunded mandate that is EMTALA (debt collectors are a separate discussion).
Green triage means that there were no reason for the patient to be in the ER. With the over-triage, green is still over 70%.
So lets presume that between red and yellows it is actually 30% and none of them are triaged up ( based on the article that I linked it seems triaged up red is high single digit which is in the same ballpark that my friends who are in emergency medicine rotation say ). Those would be the only cases where one cannot pick a non-crazy expensive service ( in fact only reds cannot, and yellow probably can which is why their service is delayed ).
So at least 70% pay 7-10x because they showed up in ER rather than in a walk in center/doctors office.
Not to be argumentative, but the stats may not be as descriptive as it might seem. I've seen kids in ER because they put popcorn in their ear and you can definitely say that they should be at the doctor's office. On the other hand, one day in the middle of the night my blood pressure spiked to 230. My heart was racing. I had no idea what was going on. I phoned the hospital and they suggested going to the ER. I did. They took an EKG and everything was normal. Diagnosis: panic attack (which I think was brought on by my previous blood pressure medicine). Doctor gave me a sedative and told me to go see my doctor the next day. I'd be in that green triage, but you don't know until after you are triaged. That's the problem.
Ironically, the next time it happened, I waited all night then went to the doctor. He sent me to the ER, who sent me right back home again. Another time, I had a friend who I suspected might be falling into a psychotic episode. They were acting a bit strange and it worried me. I got them to the ER and boy am I glad that we went. Probably saved a call to the police.
It's these kinds of things where you just don't know that are the most worrying and now that I have some experience with it, I have a much better idea of why some people park in the ER. If you've never experienced, then I am incredibly happy for you because it really sucks.
Of course I don't know that this is where a lot of these cases come from, but in my limited experience this is what I've seen. I think we need some other kind of place you can go that can triage effectively when you are worried and don't know what to do. When I was younger, I got sent to the ER because I had obviously broken my hand. That's a waste of resources. There are better places I could have gone, but if you don't know, then you don't know.
I appreciate your point but I do not think it contradicts the numbers - going to ER and getting a green triage means that the triage personnel determined that it is not an emergency.
According to 2013 National Institute of Health study put the median cost of ER visit at $1,233. In 2015 there was over 130M ER visits. Lets arbitrary assign the cost of interacting with the Triage nurse at the ER to $233 ( which is insane lets do it anyway), then the pool of cost overtriage 130M * $1000 which is $130B. Of those even triaged up 70% is a green triage, which makes it $91B.
If we are to make an assumption that for non-emergencies addressed by ER cost only twice as much non ER then simply by sending people to a regular doctor after people are getting a green triage one realizes savings of $91B/2 = $45.5B
I had my gallbladder removed in a emergency surgery over a decade ago.
It happened on a Wednesday night. I had excruciating pain, enough to nearly black out -- and a friend took me to an emergency room, where they did an ekg, ultrasound, put me on a morphine drip and operated the next day. Once the pain set in, I was in no position to do research for a variety of reasons.
I'm not sure what kind of shopping around could have taken place for that.
Could you explain how your technique would work for something like my situation?
Isn’t the solution an advanced care directive? Where you make decisions in advance of something happening, just in case you end up in a situation where you can’t decide yourself?
E.g. no extraordinary measures or no CPR, or, get me into one of these nursing homes and not this one.
Even in public health care countries, there’s plenty of decisions that are a good idea to make in advance.
I don’t see why they can’t be scaled toward cash healthcare countries.
Comparison shopping arguably isn’t the intended purpose of advance care directives—which, FYI, can only go into force if the person is legally incapitated, and being in pain, however extreme, is a grey area as I’m sure you could make the case that decision-making capacity still exists. There’s also the issue of having the agent available when such an event happens, and having them be in possession of the directive.
Anyway, even then, it’s infeasible to enumerate all the possible decisions in advance—not only is it impossible to know what your costs will be ahead of time, there’s a lot of variation in cost. There isn’t going to be a single hospital in your region that’ll have the cheapest prices across the board, so it’s not as simple as “send me to the cheapest hospital”.
It will not work for emergencies however that's not where most of the money is burned.
Most of the money is spent on non emergency medical care that can be priced using a phone or an email. That's exactly why medical tourism is possible.
It is a case of vertical capture: should you walk into a Mount Sinai hospital, the $600 MRI of Lennox Hill will cost you between $1800 and $2800. It will be done using the exact same MRI machine. The result will be sent to India probably to the exact same company that Lennox Hill sends the MRI for a radio tech readout, except that Mount Sinai MRI won't be available for 5-7 days vs. in an hour at Lennox Hill.
So why is Mount Sinai is able to charge that amount of money for an MRI? Because it is a vertical capture. Should you walk into a Mount Sinai it is extremely unlikely that you would go out of the hospital to get an MRI. They could probably charge $7,000 and still get 90% of the patients doing it.
> Personal responsibility is "hard" so no wonder those who tend to outsource it get fleeced.
What is the effect on the market when everyone engages in "personal responsibility"? If everyone finds out about Lenox Hill Radiology and goes there instead of to hospitals for MRI, won't the effect be that demand goes up without supply obviously going up, causing increased prices and wait times? What will be the effect on hospitals that were subsidizing their other business by pricing their MRIs higher?
The reason people don't like "personal responsibility" as a general-case solution is not that it's hard, but that it's not a general-case solution. This article is talking about an actual general-case solution.
Or the effect could be that Lenox Hill Radiology discovers it's getting a ton of MRI patients, has utilization above 85%, and can now afford to get another machine. A group doing a thing well getting more business is typically not a bad thing. Yes, if it's a loss leader then bad things can happen - but that doesn't seem to be the case here.
"Personal Responsibility" is just "making the market actually be a market". Markets are great - but situations where the person paying isn't the person choosing or receiving the benefit tend to be horrible in some dimension.
> What is the effect on the market when everyone engages in "personal responsibility"? If everyone finds out about Lenox Hill Radiology and goes there instead of to hospitals for MRI, won't the effect be that demand goes up without supply obviously going up, causing increased prices and wait times?
The current situation for the same MRI is:
Mount Sinai - cost $2800, wait to schedule 5 days, wait for read out 5 more days.
Lennox Hill - cost $600, wait to schedule ~1.5 hours, wait for read out, next business day.
Distance between two locations: opposite side of an avenue and half a block.
Realized savings by crossing a road: $2,200.
Where else is it possible for two identical products to be offered in that close proximity at that kind of a price difference and have people defend the pricing of the more expensive one while complaining that the services that include this product cost too much?
But here's what I think should happen: Lennox Hill would slowly increase its prices and Mount Sinai would drop its prices until it would not be possible to save $2,200 by crossing an Ave and walking for five minutes. Of course if we are to look around this is not current more likely outcome - rather Mount Sinai would buy Lennox Hill Radiology which is an independent radiology center, make it a part of the Mount Sinai hospital chain and increase Lennox Hill' price to whatever level that it currently charges ( hospital chains have been buying up independent centers hurting their cash cows for years ). Unfortunately for hospital chains radiology centers now are a proven way to make money so new ones are popping up more and more.
> What will be the effect on hospitals that were subsidizing their other business by pricing their MRIs higher?
I have never heard of this argument being used by any of the hospital chains to justify high prices for the services that can be done out of hospital and it is definitely the kind of argument that should get traction had it been possible for any hospital to bend some numbers to make it remotely plausible so I would say it is unlikely to be the case.
Did you injure yourself and went to a medical center and they told you to go to a radiology center who then told you you had an ACL injury?
I ask because at the end, you said you searched for "sports medicine surgeons" which already looks like you have _some_ knowledge about what was going on.
Which is great. But part of the problem we have is education. Most people don't even know of other options available to them and don't have the vocabulary to effectively search for what they want.
"Torn ACL" is way more specific than "Knee hurts".
Crash on a Super-G, followed by a quick prelim diagnostics of knee stability. Diagnosed as a possible tear of MCL or ACL and possible fractures.
> Did you injure yourself and went to a medical center and they told you to go to a radiology center who then told you you had an ACL injury?
You might find it interesting: all such diagnostics is actually done only using an X-rays and MRIs. Physical evaluation is just used to decide what to X-ray and what to MRI.
> Which is great. But part of the problem we have is education. Most people don't even know of other options available to them and don't have the vocabulary to effectively search for what they want.
Probably, but this is a vastly different problem from "Something unknown costs too much"
The average case where people go to the ER they don't have a week to Google and research their options. More likely minutes to hours. You can definitely find some value in the US medical system if you have the time, like coupons for prescription drugs that aren't covered.
But yes, don't go to the ER for non-emergencies and you'll save money and everyones resources. Hopefully that's basic logic to most people.
It took me three hours ( and I waited patiently for more responses ) before receiving the information and picking what seemed like an reasonable course of action. I obviously googled before to prepare myself of having my HSA wiped out. The horror stories told me it would be.[0]
In fact when the walk in center referred me to an ortho and said "It will be expensive. Here's a list of good ones" I asked if it was going to be "$800 dollar expensive?" at which point I was looked at by both the front-desk person and the Emergency medicine doctor as if I had grew two heads in front of them. They said "About 250 to see a specialist and about $800 for an MRI."
One of the two surgeons that I have selected based on their responses who could see me the next day were on the list of good ones ( ~30 ) that I was provided by the walk in center. No referral code was needed.
The surgeon offices, the walk in center and the physical therapists were having near orgasmic reactions hearing that it was going to be paid as a part of high deductible plan because it means that it is paid from a regular Mastercard as if I was a cash patient, immediately, the same day.
[0] I have taken friends to ER. They were never seen faster than 3-4 hours.
This sounds a lot like the Bitcoin Be Your Own Bank™ approach to healthcare. Being your own bank sucks. Being your own hospital is even worse. Socialized medicine can't come soon enough.
What's the incentive for me to save all that money when my insurance pays for it anyway and my company pays for my insurance? Insurance is supposed to do this job - negotiate prices ...etc., but, people are so attached to their doctors that insurance usually caves giving hospitals a much higher bargaining power.
It's a start, but imperfect because most people with a high deductible plan will also have a health savings account (HSA). The HSA may even be required, not sure. The problem with HSAs is that although it's "your" money, it can only be spent on qualified health expenses. So there's a reduced incentive to spend carefully, because you can't use the money for anything else.
> it can only be spent on qualified health expenses
Once you reach retirement age it can be used like any Traditional IRA account, except for inability to roll it over to another IRA or do a Roth conversion, if I understand correctly.
if you end up with "too much" money in your HSA, can't you just reduce the amount of money that goes into it? obviously you can't just go buy a car with the money, but to me it seems like there is a strong incentive not to overspend from your HSA if you control how much of your paycheck goes into it.
Yes, many screenings are covered 100% with no deductible. But if I think I'm having a stroke and call an ambulance, I'm responsible for the cost up to the deductible (I just checked my own HDP coverage to verify this). This wouldn't factor into my decision, but I'm fairly affluent (and my family actually maxes our deductible each year because of various chronic conditions). Someone that is in a different financial decision will absolutely be thinking of the cost of calling an ambulance (or going to the ER). Of course, if someone dies from a stroke rather than being treated and surviving, the result is lower healthcare expenditures (yes, that's morbid; but we also need to think about the incentives built-in to our healthcare system).
These were the actual costs that I have to pay out of pocket until I reach the deductible of my insurance ( yearly ). I was at zero since it is a new year. In my case it is coming out of my HSA. Basically, cash price.
That means you don’t actually know the real cost since insurance shields you from the actual amount and it can be drastically different for each insurance company. You’re just estimating with a false sense of information.
This happens in the US, too. (my daughter just had open heart surgery at a top tier research hospital.) It's very common for a resident surgeon to open the patient and prep the detailed surgical site as part of their practical work (residency, fellowship). This usually happens under direct supervision of the attending, but not always. But, in the case of cardiac surgery, "getting to the heart" is a very quick process -- a couple of incisions, some clamps & drainage, and there's a heart right in front of you. The time-consuming early part is getting the anesthesia work done (not just sedation, but installing all the necessary ports, tubes and catheters) and hooking them up on a heart/lung bypass.
We had a birth recently and the residents (who get paid very little) did 80% of the work while the attending surgeon came and went and probably spent a total of 15 minutes with us. The insurance company was still billed almost 10k for a epidural.
> how the highest skilled individuals only step in for the trickiest part of the surgery, but the simpler tasks like getting to a heart are performed by lesser doctors or nurses.
This is most certainly the case in the US. Most of teaching hospitals have residents do most of the "easy work" such as getting there, have the attending specialist perform the critical part and again have the residents do the rest.
He succesfully performed a complicated surgery for $10K that would cost $200K in the US.
And India still can't afford to pay those prices.
The problem is obviously not that THIS guy is not working efficiently. It's that the distribution of wealth under our planetary economic system is deeply unfair.
Idk if I'd agree that it's "unfair" because that implies there's some natural balance we've disrupted, when in reality wealth is largely the result of labor and ingenuity. If a group of people gets together and creates wealth for themselves and their offspring, is it unfair that they are wealthier than the rest of the population? That kind of thinking at some level is fundamentally unfair itself - if you go collect and store nuts for winter you're less likely to starve. If we say that it's unfair now that you have all these nuts and winter is coming, then how does one provide for one's self fairly?
Wealth isn't distributed, it's created. I mean you can distribute after that but it would be theft.
Nonetheless I hate that some people are just born into economic situations where they are severely less able to actuakize their potential, so I share your sentiment. I just don't like the word unfair as it seems to disregard accomplishment and to me it demonizes people who have succeeded.
Does it appeal to your sense of justice that within the same society some live opulently, yet others live in constant fear of not having the basic necessities of life? Not only would I say this is unjust, but that it is also unsound and a danger to society itself. The worst qualities of humans emerge when they are fighting for survival.
I'm fine with a system that has wealth inequality, I don't see any way around that and it's great for causing innovative pressure, but I find it hard to justify the fact that some people are deprived the basic necessities of life.
> Wealth isn't distributed, it's created. I mean you can distribute after that but it would be theft.
So are you one of those people that believe taxation is theft? Are you a self-made man? Are you Caesar without Rome? It strikes me as incredibly foolish when people ignore the fact that their success is entirely dependent upon their society.
Did you create your own school, did you create your own language ... are you really that unaware of the great debt you have to others? Without society, you'd be a degenerate caveman, you owe everything you have to it.
Actually, it doesn't strike me as foolish, it strikes me as incredibly useful for rationalizing ones station in life. It must make it easy to walk past the homeless and suffering, feeling like you are innocent and not complicit at all in the silent tragedies the system sustains.
I'll be honest - I don't know many people who are of sound mind and body and who consistently make level headed choices living in constant fear of having basic necessities. I know a LOT of people in this situation because they don't improve their skills, don't work many hours, had kids young, had numerous kids, want to live in a high demand area despite low income or because they prioritize luxury items over quality necessities. Factoring things like that in paints a very different picture than what you're saying.
Wow I thought we were having a civil discussion until the second half of your post. You have some very presumptuous nerve. Rather than responding to all the ad hominem I'll just explain:
My parents fed and clothed me for 18 years. The public services are there for a reason and many of them (ie schools) need to be there. I inherited knowledge from thousands of years of thinking. I believe all humans deserve those types of gifts, and as such I'm willing to pay my fair share back.
What I absolutely refuse is to allow people to come in and take more and more until they are satisfied. To tell me that they know better than me (as you are attempting to do) of my privilege and what I owe for it. You want to sacrifice your life's work to others? Go for it. Put your money where your mouth is. But you just keep your opinions about what I owe and what I deserve to yourself because you don't know me and I guarantee you're going to look like an idiot if you continue to try to talk down to me.
> I know a LOT of people in this situation because they don't improve their skills, don't work many hours, had kids young, had numerous kids, want to live in a high demand area despite low income or because they prioritize luxury items over quality necessities.
Yes, of course. Are you suggesting all people are wise and have this foresight? Are you suggesting that people aren't raised in stressful and violent environments, greatly worsened by economic pressure, whom turn to vice instead of education and productivity? I don't think it paints a different picture, I think it reaffirms my position: that some people aren't fit to thrive in society, but that doesn't mean (by my values) they do not have the RIGHT to the necessities of life.
> To tell me that they know better than me (as you are attempting to do) of my privilege and what I owe for it.
This is not a matter of logic, but of principles. I do not believe I know better than you, I believe I understand the plight of common people more than you, and that my view of the world has been formed by that. You aren't wrong, I'm not wrong. I know this, but at the same time rhetoric which casts the proponents of opposite principles as being in the wrong is the main tool one has in convincing others that his principles are the "right" ones.
> I guarantee you're going to look like an idiot if you continue to try to talk down to me.
I'm sorry I rustled your jimmies so much. It's not personal, I was just addressing the position you seemed to be defending. I only know you as a paragraph of text, take it easy.
See you're still trying to be condescending. You don't know me and you made all those lurching assumptions. You asked insulting questions and tried talking down to me. Enjoy your feeling of superiority.
“For we each of us deserve everything, every luxury that was ever piled in the tombs of the dead kings, and we each of us deserve nothing, not a mouthful of bread in hunger. Have we not eaten while another starved? Will you punish us for that? Will you reward us for the virtue of starving while others ate? No man earns punishment, no man earns reward. Free your mind of the idea of deserving, the idea of earning, and you will begin to be able to think.”
"that implies there's some natural balance we've disrupted"
There's a whole history of colonialism to contend with. What was once nearly a quarter of world GDP in 1700 dropped to less than 5% in 250 years. The whole country was deindustrialized.
It's a lot easier to actualize our potential in some places. I don't think it's demonizing me to admit that if I was born a woman in Sub-Saharan Africa, or in a war zone, I wouldn't have been able to build wealth like I have.
> The fundamental assertion of capitalism is that capital should beget capital.
This quote explains just half the story. The half of the story being: "success".
Pray tell me how is wealth created by labor without someone investing the necessary capital required to begin with? It is not like the labor worked for free.
The "wealthy" laboured at one point to earn that capital. They just "chose" to invest their hard-earned capital wisely which helped them beget more capital. Upto that point, your assertion holds true.
There are many who were "wealthy" who made blunders when they did not invest their capital wisely and lost it all. Would the fundamental assertion of capitalism "capital should beget capital" hold true in this case? And for all the Zuckerbergs, Jobs and Gates out there, there are a million more who failed. Those million are proof that the fundamental assertion of "capital should beget capital" is false.
The only assertion that fits Capitalism is "Survival of the fittest". I can live with that!
Trick of the wealthy. It's the only thing that keeps people from revolting against this madness. Donald Trump's fortune is largely the result of labor and ingenuity, right? This warped perspective is going to be the death of us.
The aspect of capitalism that's problematic to me is not that people can generate wealth through labor, it's that they can generate wealth through wealth.
You can make far more money just by being rich and owning capital than you ever can by your own labor. You can own physical property that makes money like farmland, apartment buildings, natural resources, factories, etc. or you can be a shareholder in companies which make money.
Either way, it's not really your labor that's making you richer, and that's the part that feels unfair about the whole system.
I agree to some extent that wealth begetting wealth can be problematic, but in order to have the first bit of wealth someone has to create it. If you made the first hammer you'd be able to make more hammers much easier. You've effectively made the world wealthier by your work and invention and as a result it's fair that you get more than just the value of your hammer.
Your claim about making more wealth from wealth than labor kinda skips over the parts about needing so much wealth and having to accumulate it.
War and genocide have been part of human history since before the split from chimpanzees. Wealth in anything like what we’d recognise it dates to after the rise of agriculture.
We can be quite confident that European wealth during the age of colonialism didn’t have much to do with colonialism as such because that wealth preceded the colonies and neighbours that differed in having colonies were much the same economically. Britain was rich before it took over India. Germany had no colonies of any economic importance and Austria-Hungary none. They do not suffer by comparison with France with its extensive colonial empire.
True, but it's the distribution of wealth _between_ the U.S. and India that I'm thinking of. They can't afford to give most of their population needed heart surgery even when they've made it 100x cheaper than it is here.
Here health care is destroying us too, but _most_ (not all) people who need heart surgery still get it. Sometimes it destroys them financially (not saying health care works here either), but they get the surgery. And our economy does not crash. So far. India literally can't afford to give them the surgery.
>India literally can't afford to give them the surgery.
This is what's hard to conceptually grasp about nationalized healthcare. The concept of "a nation can't afford" does not make sense because a nation-state with control of its own currency can simply create and allocate the currency to serve this purpose.
I originally thought this comment deserved downvoting, because "we'll just print money" shows a lack of understanding about the role fiat currency plays in an economy. However, I realized that this comment is a valuable addition to the discussion, because it expresses an increasingly common misconception.
So thanks for posting it.
Yes, the nation can just print money, but will anyone accept it?
When the supply of money increases, but economic output and resources are held constant, prices increase.
Imagine if the resources available in the economy are worth M currency. If the government just creates 10M currency, that doesn't mean more things are available to buy, just that each unit of currency is now only worth 1/10 of what it was before, so prices rise. But because people expect that, they try to get rid of the currency even faster, so prices rise even more than the increase in the money supply.
This results in "hyperinflation" - prices rising more than 50% per _month_ - see https://en.wikipedia.org/wiki/Hyperinflation for accounts of governments who have tried the "create and allocate currency" approach.
There's a great "Planet Money" episode on the hyperinflation of Brazil, which started when the country decided they could just print money to build a beautiful new capital city, and how it persisted for decades because it destroyed people's faith in the currency as a store of value, until Brazil created a new stable currency and convinced people they would no longer just print money to spend. https://www.npr.org/sections/money/2010/10/01/130267274/the-...
I knew I'd get this kneejerk reaction to "simply create and allocate the currency," I was holding out hope that responders would finish reading the sentence.
What I said was:
>a nation-state... can create and allocate the currency to serve this purpose.
I totally agree with you in a general sense. Creating and allocating currency and distributing it to the general population equally will cause the scenario you describe. "More dollars chasing fewer goods," as Greenspan described[1].
However, if we take the hypothetical scenario that the government agrees to pay exactly the current cost of the procedure at Narayana for medical procedures, none of what you described will come to pass. Wait times at Narayana might increase because more people might come in to have the services performed, but it will not cause runaway across-the-board inflation.
The point is that inflating the money supply is a tax, just a hidden one spread across all holders of assets denominated in that currency (cash, loans, salaries, ...)
Smaller amounts of "print and spend" inflate less than large amounts, but they do cause inflation, and the wish list is never just healthcare.
Controlling a fiat currency lets you hide some taxation as inflation, but it is no free lunch.
It is no free lunch, but I never claimed it was. It is an option on the table, not one without consequences.
It’s never just healthcare, sure: move the goalposts and set up your slippery slope.
But consider this: what if the tax produced value over the cost of its implementation? What if it prevented harder, more expensive downline complications or made the population more productive—more likely to gain, retain and apply their education?
What if we looked to it as an investment in our people?
Proposing that it is a justifiable tax for investment is very different from saying "the concept of 'a nation can't afford' does not make sense [for] a nation-state with control of its own currency".
It looks like you understand why even a nation that controls it's own currency may not be able to afford nationalized healthcare:
1) because creating and allocating currency inflates prices, it just hides the cost rather than eliminating it
2) because we cannot eliminate the cost by creating currency, cost and benefit of healthcare spending must still be evaluated in comparison to other spending priorities
No, I disagree. The money represents the real output of the economy. This can be moved around to some degree (switch a bicycle factory to making surgical tools, etc) but fundamentally only so much stuff is produced. Printing more money doesn't change this.
Economic growth does, but not overnight. And figuring out how to do equivalent things with less input (whether it's model-Ts, or surgery) is an important part of that.
To take an extreme example, every space-X launch costs $50 million. If I say that America could not afford to give everyone an orbital holiday, this is not a statement about fiat dollars. It's a statement about the enormous resources, and chiefly the labor of an enormous team of people (including all the suppliers, and their suppliers) required for each such trip.
> The concept of "a nation can't afford" does not make sense
Of course it makes sense. In any healthcare system (yeah, even pricate insurance) there are tradeoffs to be made, because the reality is that resources (hospitals, doctors, time, not necessarily just money) will always be finite. For example, having a breast scan every year might save more people than having it every 5 years, but at some point the marginal returns will be so small that it makes more sense to focus resources on other things.
Because money is just a proxy for resources. Printing more money does not create more of everything else, so it drives inflation and effectively acts as a tax on all other economic activity. You can print more, but you need to be aware that what you are doing has that effect, and if you overdo it you'll cripple your economy just the same as if you increase tax rates too much.
The natural distribution of wealth, on the other hand, is eminently fair. Before agriculture everyone was poor. After the rise of agriculture almost everyone was poor but there were many more of them, and those who were “not poor” had no medicine worth the name, could not travel with anything resembling modern convenience and lived in the dark when the sun went down. Starting sometime between 1300 and 1800, depending on measurement the first sustained rise in living standards in human history began, because of capitalism.
It’s how almost all other sustained rises in living standards have happened too. China’s first growth miracle in the 20th century happened because going from civil war to the Communist Party was an improvement but in India, China, Indonesia, Russia, moving to capitalism lead to a rise in living standards.
Fairness would be nice but let’s try getting everyone out of poverty first.
I had a history professor tell me that if there was any kind of cultural/economic revolution in the US, it would be over health care. And that was during the worst of the HMO days.
It's even worse now with these "HMO/PPO hybrid" systems, where instead of getting nothing, you get "something", then a massive hospital bill afterwards.
> The data appear to back Shetty up. In part because its huge volumes help surgeons quickly develop proficiency, the chain’s mortality rates are comparable to or lower than those in the developed world, at least for some procedures. About 1.4 percent of Narayana patients die within 30 days following a heart bypass, according to the Commonwealth Fund, which studies public health, compared with 1.9 percent in the U.S. Narayana also outperforms Western systems in results for valve replacements and heart-attack treatment, the group found.
I’d always heard that although the US’s healthcare is the most expensive, it also has the best outcome for specialist care. But the fact that this hospital outperforms the US while charging a fiftieth as much makes me wonder how much better the specialist care could be outside of the US given the same resources.
One of the most interesting discoveries in US medicine is that there is essentially no relationship between cost and outcomes- even within the US. The Dartmouth Atlas of Health Care has shown that there are wide price disparities within the US (and not necessarily in predictable ways, e.g. https://www.newyorker.com/magazine/2009/06/01/the-cost-conun... ) and that they don't correlate with improved outcomes. To some extent, prices are a random walk that is orthogonal to a different random walk that is 'quality.'
Then again, repetition helps. People who do more procedures generally get better results. In colonoscopies, studies show that the fastest doctors also have the lowest false positive/negative rates, because the way you get fast and the way you get good is to do it again and again.
My wife fainted at a Shake Shack in NYC on the UWS. The 5 hour hospital stay with medicine, a regular check in from a nurse, and fluids cost less than $500. The < 5 MINUTE ambulance ride cost over $2500 to go from W77 to E77 (straight across the park, about a mile).
Well, you need to just appear to not be sick and they'll accept you as a ride: don't barf allover the place as you get in, wait until the trip has started. After that, they have every incentive to deliver you to the hospital.
Sure, ideally we'd have reasonable ambulance pricing, but since that's not going to happen, taxis and ubers/lyft are the best thing.
Me = goto ER for absurdly high BP and heart palpitations, which I've never had before. Quick hook up to ekg, watch BP, learn about PVCs, get kicked out after an hour or so as BP lowers somewhat. All in the hallway, no real admission. Admittedly not necessary looking back but you do what you have to.
Cost? $10k for the ER. $1500 for the doctor.
Next cost? $4k for the ER if I'm poor
Next cost? $350 of co-pay once I dug out my insurance card, God knows what Blue Cross pays.
Broken system? I think so.
Actually it wasn't a critically urgent problem but needed doctors attention. If someone wants an idea for an app or website - a way to lookup local ERs by price would be great.
Last year my system cut her finger quite deeply while dealing with a can opener, at ~9.30pm. It wasn't an ambulance-worthy emergency but still, it didn't look good. So we called our emergency number and they sent out an "ambulance lite", basically a paramedic and a doctor who's just finished university.
The cut wasn't serious despite the great loss of blood, but it was in a tricky spot and the young doctor didn't want to deal with it without a second opinion. So they took her to the ER, and we followed by car.
At the ER, within 45 minutes, she had seen the doctor on call that night and got the stitches put on from the cosmetic surgeon on duty that night.
Not only it didn't cost us 1 cent but we even got a free cup of coffee out of it, offered by one the ambulance drivers who was on call that night.
I envy a lot of things about the US, but not their medical care.
My fear is that if hospitals start to make their prices publicly available, it will drive prices upward not downward.
Why? Because hospitals have no incentive to compete on price. The majority of people get ambulance'd to the nearest hospital, not necessarily the cheapest one.
So any hospital that notices it's charging less than its competitors will raise its price, because, why not? It's a very inelastic demand.
Er, and, most folks arrive by car. I'm pretty sure ambulance arrivals are a tiny percentage of their overall business.
Opinion based on a. Being alive and b. Paying accident claims for 5+ years.
Even with accidents, most claims did not involve an ambulance bill. In one memorable claim, a gunshot victim drove himself to the ER with multiple bullet wounds while bleeding profusely.
that is the whole point of publishing prices. with it implicitly you have to adjust your billing to be able to charge predictably for a service such as MRI etc. and if you dont you dont survive in long run as people gravitate towards the providers that give them clarity.
why should be hospitals be the only ones allowed to do this highly anticompetitive practice?
If clarity was a compelling concern for healthcare purchasers, everyone would buy HMO plans, which provide certainty for most things even where the provider doesn't.
And an app to verify that all doctors, nurses and equipment used in a procedure are all part of your in-network. Going out of network is so devastating, you could loose your entire life savings.
I've read about this "assembly line surgery" being tried in the US as well. But the purpose was to experiment with replacing some of the more junior doctors with technicians. For example, there would be a technician who is only trained in opening the chest for heart surgery. That would be all they do, going from room to room opening chest cavities. Another technician would only do suturing at the end. These technicians would not be doctors, they would be folks who would get about as much training as an EMT (about 150 hours).
The next step after that is replacing the technicians with robots.
The only downside to this system (robots or technicians) is how will you ever get experienced doctors to do the hard stuff if they never get to practice doing the routine stuff first?
I’ve worked as a surgical technician and can say that this already occurs in most hospitals. It was within my scope of practice to help the doctor suture at the end of the case as well as apply staples and bandaging so that they didn’t need to.
> The only downside to this system (robots or technicians) is how will you ever get experienced doctors to do the hard stuff if they never get to practice doing the routine stuff first?
I think this argument applies to any kind of progress. As technology evolves, society loses skills, but the net benefit is hugely positive. Eventually, we don't even remember that the skills we lost were skills we once had. We get by.
This is a bonafide question as I really don't know.
Could you train a surgeon without them ever being a doctor? Basically extract out the knowledge they need and train simply for that? It seems to me that the natural skills needed might be very different than those you need to make it through a typical medical school + a career as a family doctor.
Not only that - not all hospitals follow this assembly line, if this chain of hospitals goes under what about the opportunities for someone doing the routinely 1 part of the surgery.
One of the bigger problems I observed in the US is a defensive approach against being sued by the patient. The doctor prescribes a battery of tests even though he is more or less sure what the symptom might be. But let's play it safe and not get sued approach to everything! Healthcare professionals carry insurances in millions against being sued. The cost ultimately gets passed on to customers. Accountability is good, but not at this cost! At the other end of the spectrum accountability is much harder in a country like India hence the incentive to take risks.
The problem I see in the US is a defensive approach against being sued by the patient. The doctor prescribes a battery of tests even though he is more or less sure what the symptom might be. But let's play it safe and not get sued! Healthcare professionals carry insurances in millions against being sued. This ultimately gets passed on to customers. Accountability is good, but not at this cost!
The hospital or larger healthcare organization derives real monetary value from the prescribing of these tests, I don't think it all boils down to "cover your ass". In a lot of cases it's to charge more per patient.
The moment teacher sowed the seed of change: "But his attitude to school changed drastically in 1967, when a teacher informed the class that a South African doctor had just performed the world’s first heart transplant."
I applaud the ends but I'm not sure I'm comfortable with the means.
In circles where discipline is valued, rote tasks aren't worthless. Considering them to be beneath you can be a trap.
Those easy steps help keep you centered on your craft. They might even give you time to prepare for what comes after. Taken too far they can rob you of the time to pursue skill advancement, sure. But eliminating them completely? I think that will turn out to be a mistake in ways we can't anticipate (possibly very different from the concerns I already stated above).
>Narayana has been able to get the retail cost of a heart bypass, its most common operation, down to $2,000, about 98 percent less than the U.S. average.
I'd like to see where they got these numbers. The average Medicare payment for DRG 236 (Coronary Bypass without Cardiac Catheter and without MCC) is $23,500. Something doesn't add up here. After adjusting for wage differences I'd imagine the numbers are much closer than this article implies.
There are non-assembly line private hospitals which cost 4x. Narayana doens't have AC rooms (OTOH) and otherwise cuts cost:
> right from design and construction, Narayana Hrudayalaya has sought new ways to cut costs. It has kept the design compact, reduced empty spaces and used prefabricated structures. Also, instead of marbles and expensive furniture, the hospital has used simple tiles and low-cost seating, reducing the cost per bed to Rs 12-18 lakh, compared with Rs 60-80 lakh at other corporate hospitals.
I think applying methods that for manufacturing to healthcare is not a good idea. Manufacturing is generally very predictable whereas health care often isn't. We already have tried to manage software development like an assembly line. That didn't work for software and I don't think it will work for health care.
> I think applying methods that for manufacturing to healthcare is not a good idea. Manufacturing is generally very predictable whereas health care often isn't.
"- developers pick them, implement them, and put them up for review"
In quite a few cases it turns out that it's not so easy to implement what you thought first because there is a bug in some system you are using or some other component needs to be changed too and suddenly the whole plan falls apart. There is no amount of planning you can do to avoid this. Unexpected things come up all the time.
I am not saying that health care can't improve but by nature it's much less predictable than manufacturing a car.
I think I am uniquely positioned to refute your claims.
I was a mechanical engineer at an automobile company before moving to software.
The two are actually quite similar.
It is common to run into implementation issues when going from concept to production.
The big difference is, being a mature branch in an area where safety is vital, the rigor, scrutiny and time alloted to each step are significantly greater than software.
The similarity is especially pronounced on enterprise software products that have long intervals between releases.
A lot of unexpected things happen with cars that go into production all the time. Thankfully cars have a lot of redundancy required by safety. So, small problems can often be glossed over.
"I was a mechanical engineer at an automobile company before moving to software. The two are actually quite similar"
Me too :-)
Yes, things happen when you get something in production but at some time you reach a fairly stable state and things are predictable and easy to measure and quantify. With medical procedures you often encounter surprises.
I agree there is something to learned but it would be terribly arrogant to say "We have figured it out for cars and therefore we have figured out medical care and software development"
I am pleasantly surprised. Always nice to see people who have made such a transition.
I agree with you on all points here. Once in production, stability is achieved and car companies certainly do not hold all the secrets to resource allocation and administrative approaches to healthcare.
The degree of unpredictability is higher in software and medical procedures.
The supply chain - production approach can only get so far.
That being said, the production approach can work splendidly well for low risk diagnoses. The production approach has already been adopted by some software companies. Especially contract based companies that involve a well defined repetitive grind and set of tools. Think developing a Cash-of-clans like mobile game or making websites for certain organizations. Both industries are quite mature. The software problem isn't interesting, but it also rarely throws curve balls.
_______
I am going on a slight tangent, but here goes.
I think there are some medical low hanging fruits. This is especially true in the US, where the escalation of service is extreme. Either you get no service or a $200/hr medical expert.
If the disease is going to be a low risk common illness 95% of the time, then maybe the patient could go through a $40/hr medical practitioner whose job would be to attends to 'easy' cases and only escalates it to the $200/hr doctor if the case is serious enough.
A similar case applies to the ER and ambulances too. There is, "I am about to die" emergency and then there is the "I am hurt, but 20 more minutes to the hospital in car won't change much" type of emergency.
Off topic: But, This approach is quite similar to a popular ML approach called Cascade Classifiers used for resource efficient applications. It is apt, that it would come up in a discussion about how to make Healthcare more resource efficient.
Lastly, I find the requirement of 4 year college to enter medical school to be preposterous. It is a waste of money and time for applicants and serves only to line pockets of academic institutions.
Assembly lines are great for building from scratch. However, no two humans are alike. It's similar to the difference between greenfield and maintenance software development.
There are much less drastic things that could be tried, but I don't see much political will for real change. We get a lot of talk, but few concrete plans.
to me what Shetty shows is how the power of smart and thoughtful entrepreneurship can not only thrive profit-wise, but can produce results that benefit for everyone even in such high risk (surgeries), low reward (large chunk of clientele appears to be made of India's lower income population) industry
I don't think one could naively apply his methods to the US healthcare system and get the same results, but what he has done at least demonstrates once again that the healthcare system is likely irrevocably broken
Some equipment is too expensive to be disposable and therefore requires enhanced cleaning protocols[0], but reusing as much equipment as possible just to save a few bucks seems penny wise but pound foolish. Why add unnecessary risk [1] if you can easily avoid it?
Meanwhile, people in Sub-Saharan Africa manage to feed themselves on less than a dollar a day. They must have a much more efficient food delivery system than our own.
It sounds like a bad idea - but scalpels and metal tools are not thrown away either - they're sterilized. Something like a plastic tube may have 2 or 3 uses in it instead of just 1 - as long as the sterilization is within acceptable tolerances - why not? A reusable rocket too was unthinkable until a private company did it. One shouldn't discard experimental evidence just because it conflicts with one's belief systems.
Good article that raises some very good questions. I had a few specific takeaways out of it.
>“Everyone does as much as they can,” Ashwinikumar Kudari, a senior gastrointestinal surgeon, says toward the end of a busy day at the Bangalore hospital. He’s just removed two malignant tumors the size of golf balls from a middle-aged woman’s intestines—the seventh surgery he’s performed or supervised since morning. A compact man with a trim mustache and a wry smile, Kudari is soon on the move again, checking in briefly on a gallstone removal next door before dashing up a spiral staircase to another operating theater. There, he takes over from a colleague who’s struggling to locate a particularly tricky fistula. “Our margins are low on one surgery, but because we do so many in a day, we can make enough,” he remarks after the elusive fistula—the longest he’s ever seen—is found, running from the man’s anus to above his groin. By working at this pace, the average Narayana surgeon performs as many as six times more procedures annually than an American counterpart.
I'm wondering how overworked doctors are in these conditions, or how long a senior doctor lasts in a hospital like this. It might be a good place to gain experience, but how feasible it is to work there for 10 years?
>It’s all a far cry from the high-touch treatment Westerners expect, but Shetty is adamant that none of the practices compromise safety. Sterilizing and reusing clamps and tubing is permitted under the standards of the Joint Commission, a U.S.-based body that vets and accredits hospitals worldwide, including Narayana’s cardiac hub. Involving properly instructed family members in the simplest care tasks isn’t unheard of in Europe and North America, and some studies suggest it may improve patients’ prospects. (Unlike busy nurses, relatives have just one person to focus on.)
I growing up in the soviet block I remember family members taking care of relatives in the hospital, and I never really questioned this at that time. Now looking at the western medical system, it seems like nurses are doing work that there not supposed to be doing and there aren't enough of them all the time.
> Yet even for bypasses—Narayana’s bread-and-butter procedure, with greater economies of scale than any other—Shetty needs to cut costs further, because Modicare will reimburse only about $1,300 for each surgery. For other treatments, the difference between current price tags and Modicare payment schedules is much wider. “They are paying less than what it costs,” Shetty says.
It seems that politicians have established a system that covers everyone. Not always effective, that underpays a lot, but it's there, now as society gradually accepts that the system is their and it is fair, it may be possible to expand in in the next 5-10 years either with the amount of coverage it provides or with the amount of money it pays per procedure.
In UK you are using NHS, a public service, funded out of your tax dollars. NHS spent over £124.7B in 2017/2018 so your average cost is about £2000/person. Not sure how you can break out costs for heart bypass but I suspect they will be much more than $2K/surgery. Narayana Hospital is private and has been profitable continuously, with $8M profit in 2017. And still their patient mortality rate is lower than the US (1.4% patients die within 30 days after heart bypass, compared to 1.9% in the US).
Somebody is paying, and even if you're not paying out of pocket it definitely matters how much the government is paying and economizing, because they have to stretch your tax dollar/pound too.
That's why I said "(directly)". But yes I agree with your point.
Its unclear to me whether figures quoted are prices you pay, or cost to do the procedure. Some at least appear to be the price you pay ("Shetty did it for about $10,000 and turned a profit"), which as I don't pay anything directly, suggests that they need to qualify 'cheapest'.
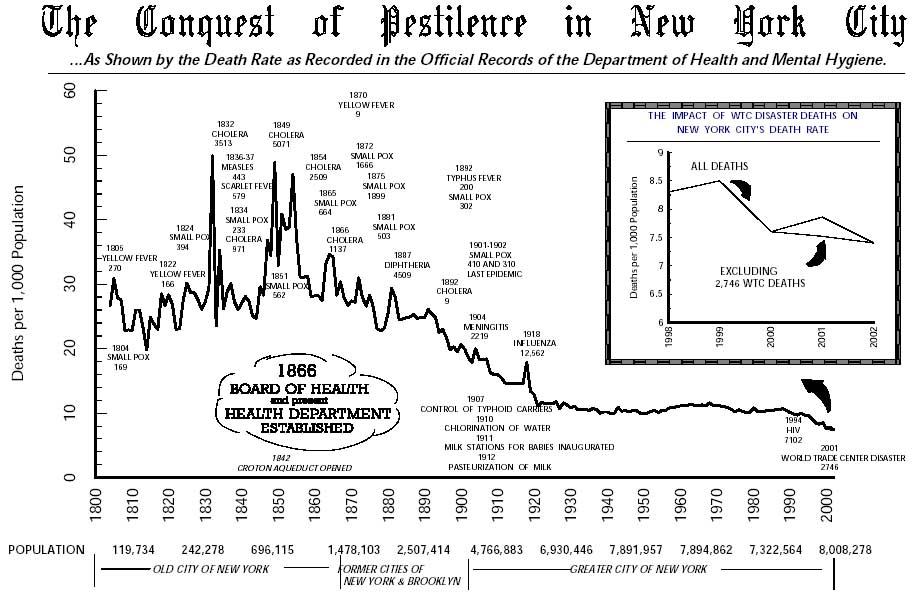{kind=link}
FWIW, I'm relatively well off and have medical insurance, but the cost is absolutely negligible compared to what I hear is prevalent in the US - about $10 / month.
It's probably just my bad luck, but I've had three surgeries in the last 10 years - an appendectomy, an ACL replacement, and a septoplasty. Each one of these was done in highly regarded (and expensive) hospitals in Delhi - Apollo, Max, and Fortis. Each time I walked out of the hospital without paying a single dime. I just had to show my insurance card, and the entire stay was cashless. In fact, after my last surgery I realised that I could have even been reimbursed for my medication post surgery if I'd kept the receipts (which I unfortunately didn't).
Anyhow, more power to Narayana.